Department of Cardiology, University Heart Center, University Hospital Zurich, Rämistrasse 100, 8091 Zurich, Switzerland.
Center for Translational and Experimental Cardiology (CTEC), Department of Cardiology, Zurich University Hospital and University of Zurich, Rämistrasse 100, 8091 Zurich, Switzerland.
Eur Heart J. 2024 Jan 7;45(2):89-103. doi: 10.1093/eurheartj/ehad486.
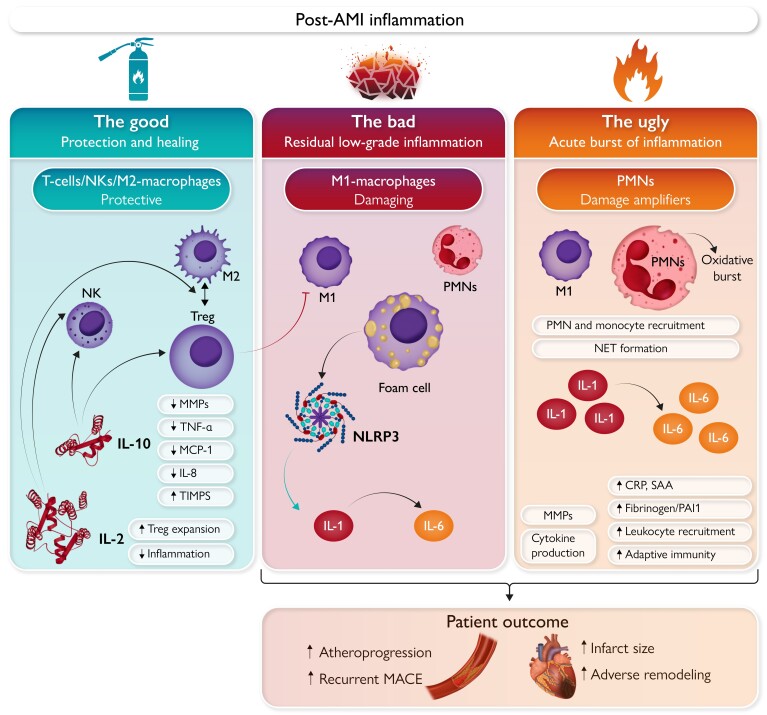
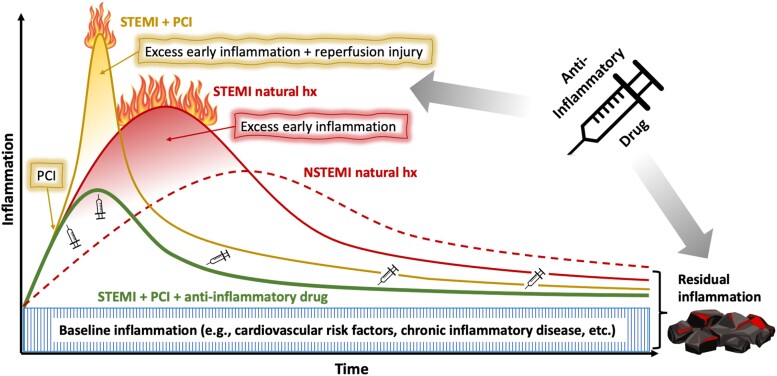
Convergent experimental and clinical evidence have established the pathophysiological importance of pro-inflammatory pathways in coronary artery disease. Notably, the interest in treating inflammation in patients suffering acute myocardial infarction (AMI) is now expanding from its chronic aspects to the acute setting. Few large outcome trials have proven the benefits of anti-inflammatory therapies on cardiovascular outcomes by targeting the residual inflammatory risk (RIR), i.e. the smouldering ember of low-grade inflammation persisting in the late phase after AMI. However, these studies have also taught us about potential risks of anti-inflammatory therapy after AMI, particularly related to impaired host defence. Recently, numerous smaller-scale trials have addressed the concept of targeting a deleterious flare of excessive inflammation in the early phase after AMI. Targeting different pathways and implementing various treatment regimens, those trials have met with varied degrees of success. Promising results have come from those studies intervening early on the interleukin-1 and -6 pathways. Taking lessons from such past research may inform an optimized approach to target post-AMI inflammation, tailored to spare 'The Good' (repair and defence) while treating 'The Bad' (smouldering RIR) and capturing 'The Ugly' (flaming early burst of excess inflammation in the acute phase). Key constituents of such a strategy may read as follows: select patients with large pro-inflammatory burden (i.e. large AMI); initiate treatment early (e.g. ≤12 h post-AMI); implement a precisely targeted anti-inflammatory agent; follow through with a tapering treatment regimen. This approach warrants testing in rigorous clinical trials.
已有的实验和临床证据表明,促炎途径在冠状动脉疾病的病理生理学中具有重要作用。值得注意的是,人们对治疗急性心肌梗死(AMI)患者炎症的兴趣已从慢性方面扩展到急性阶段。少数大型临床试验已经证明了通过针对残余炎症风险(RIR)(即 AMI 后晚期持续存在的低级别炎症的余烬),靶向抗炎疗法对心血管结局的益处。然而,这些研究也让我们了解了 AMI 后抗炎治疗的潜在风险,特别是与宿主防御受损有关。最近,许多规模较小的试验已经探讨了在 AMI 后早期靶向过度炎症有害发作的概念。这些试验针对不同的途径并实施了各种治疗方案,取得了不同程度的成功。来自于干预白细胞介素-1 和 -6 途径的这些研究的结果令人鼓舞。从这些过去的研究中吸取经验教训,可以为针对 AMI 后炎症的优化方法提供信息,这种方法可以针对“坏”(持续性的 RIR)进行治疗,同时保留“好”(修复和防御),并抓住“丑陋”(急性阶段过度炎症的爆发)。这种策略的关键组成部分可能如下:选择具有大的促炎负担的患者(即大的 AMI);尽早开始治疗(例如,AMI 后≤12 小时);实施精确靶向的抗炎药物;采用逐渐减少的治疗方案。这种方法需要在严格的临床试验中进行测试。