Department of Radiology, Beijing Ditan Hospital, Capital Medical University, No. 8 Jingshun East Street, Chaoyang District, Beijing, China.
BMC Gastroenterol. 2023 Aug 17;23(1):285. doi: 10.1186/s12876-023-02920-2.
Acute-on-chronic liver failure (ACLF) is a syndrome with high 28- and 90-day mortality rates. Magnetic resonance imaging (MRI) has been widely used to diagnose and evaluate liver disease. Our purpose is to determine the value of the imaging features derived from Gd-DTPA-enhanced MRI for predicting the poor outcome of patients with ACLF and develop a clinically practical radiological score.
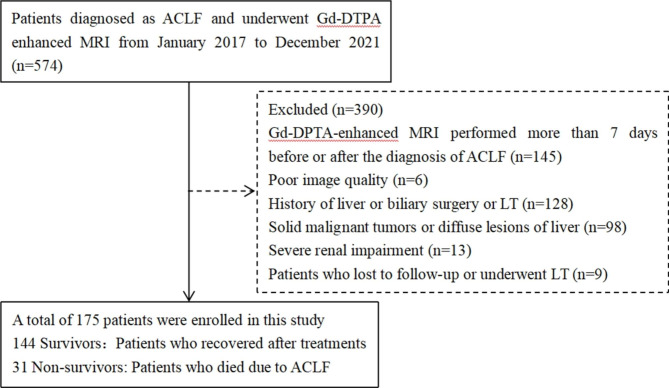
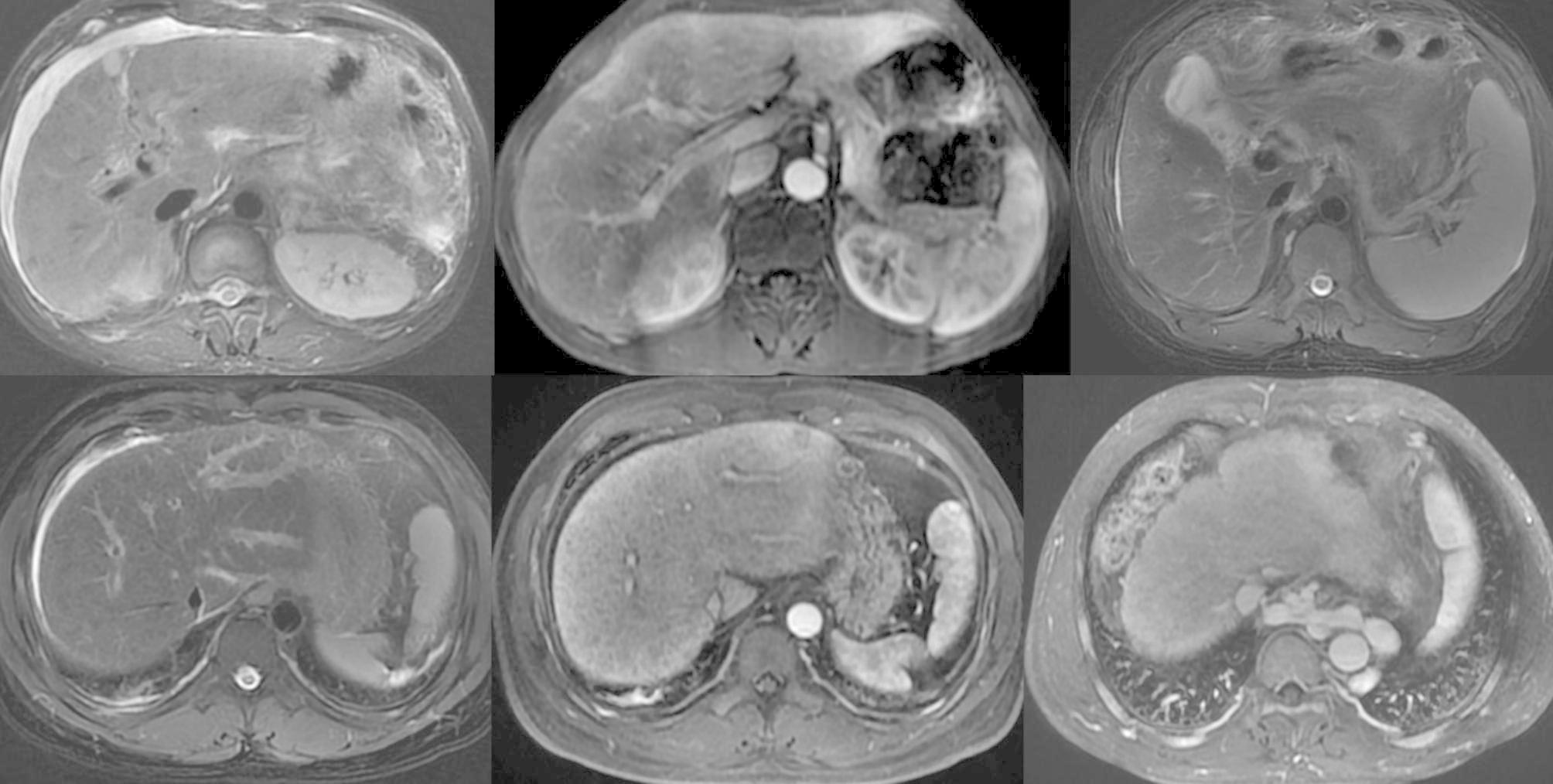
This retrospective study comprised 175 ACLF patients who underwent Gd-DTPA-enhanced abdominal MRI from January 2017 to December 2021. The primary end-point was 90-day mortality. Imaging parameters, such as diffuse hyperintense of the liver on T2WI, patchy enhancement of the liver at the arterial phase, uneven enhancement of the liver at the portal vein phase, gallbladder wall edema, periportal edema, ascites, esophageal and gastric varix, umbilical vein patefac, portal vein thrombosis, and splenomegaly were screened. Cox proportional hazard regression models were used to evaluate prognostic factors and develop a prediction model. The accuracy of the model was evaluated by receiver operating characteristic (ROC) curves.
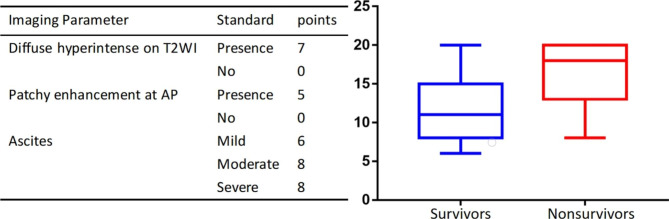
During the follow-up period, 31 of the 175 ACLF patients died within 90 days. In the multivariate analysis, three imaging parameters were independently associated with survival: diffuse hyperintense on T2WI (p = 0.007; HR = 3.53 [1.40-8.89]), patchy enhancement at the arterial phase (p = 0.037; HR = 2.45 [1.06-5.69]), moderate ascites (vs. mild) (p = 0.006; HR = 4.12 [1.49-11.36]), and severe ascites (vs. mild) (p = 0.005; HR = 4.29 [1.57-11.71]). A practical radiological score was proposed, based on the presence of diffuse hyperintense (7 points), patchy enhancement (5 points), and ascites (6, 8, and 8 points for mild, moderate, and severe, respectively). Further analysis showed that a cut-off at 14 points was optimum to distinguish high-risk (score > 14) from the low-risk group (score ≤ 14) for 90-day survival and demonstrated a mean area under the ROC curve of 0.774 in ACLF patients.
Gd-DTPA-enhanced MR imaging features can predict poor outcomes in patients with ACLF, based on which we proposed a clinically practical radiological score allowing stratification of the 90-day survival.
慢加急性肝衰竭(ACLF)是一种具有高 28 天和 90 天死亡率的综合征。磁共振成像(MRI)已广泛用于诊断和评估肝脏疾病。我们的目的是确定 Gd-DTPA 增强 MRI 得出的成像特征在预测 ACLF 患者不良预后中的价值,并制定一种临床实用的影像学评分。
这项回顾性研究纳入了 2017 年 1 月至 2021 年 12 月期间进行 Gd-DTPA 增强腹部 MRI 的 175 例 ACLF 患者。主要终点是 90 天死亡率。筛选出 T2WI 上弥漫性肝脏高信号、动脉期肝局灶性增强、门静脉期肝不均匀增强、胆囊壁水肿、门周水肿、腹水、食管胃静脉曲张、脐静脉扩张、门静脉血栓形成和脾肿大等影像学参数。使用 Cox 比例风险回归模型评估预后因素并制定预测模型。通过受试者工作特征(ROC)曲线评估模型的准确性。
在随访期间,175 例 ACLF 患者中有 31 例在 90 天内死亡。在多变量分析中,三个影像学参数与生存独立相关:T2WI 上弥漫性高信号(p=0.007;HR=3.53[1.40-8.89])、动脉期局灶性增强(p=0.037;HR=2.45[1.06-5.69])、中量腹水(与少量相比)(p=0.006;HR=4.12[1.49-11.36])和大量腹水(与少量相比)(p=0.005;HR=4.29[1.57-11.71])。基于弥漫性高信号(7 分)、局灶性增强(5 分)和腹水(轻度、中度和重度分别为 6、8 和 8 分),提出了一种实用的影像学评分。进一步分析显示,在区分高危(评分>14)和低危(评分≤14)组 90 天生存率方面,截断值为 14 分是最佳的,在 ACLF 患者中,ROC 曲线下面积的平均值为 0.774。
Gd-DTPA 增强 MRI 特征可预测 ACLF 患者的不良预后,在此基础上,我们提出了一种临床实用的影像学评分,可对 90 天生存率进行分层。