Department of Obstetrics, Birth Center Wilhelmina Children's Hospital, Division Woman and Baby, University Medical Center Utrecht, Utrecht, the Netherlands.
Department of Biostatistics and Research Support, Julius Center for Health Sciences and Primary Care, University Medical Center Utrecht, Utrecht, the Netherlands.
Acta Obstet Gynecol Scand. 2023 Nov;102(11):1521-1530. doi: 10.1111/aogs.14643. Epub 2023 Aug 18.
The majority of data on COVID-19 in pregnancy are not from sound population-based active surveillance systems.
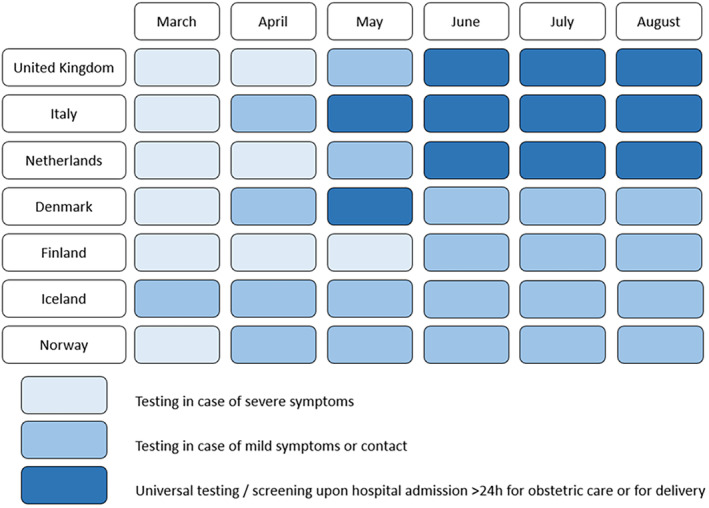
We conducted a multi-national study of population-based national or regional prospective cohorts using standardized definitions within the International Network of Obstetric Survey systems (INOSS). From a source population of women giving birth between March 1 and August 31, 2020, we included pregnant women admitted to hospital with a positive SARS-CoV-2 PCR test ≤7 days prior to or during admission and up to 2 days after birth. The admissions were further categorized as COVID-19-related or non-COVID-19-related. The primary outcome of interest was incidence of COVID-19-related hospital admission. Secondary outcomes included severe maternal disease (ICU admission and mechanical ventilation) and COVID-19-directed medical treatment.
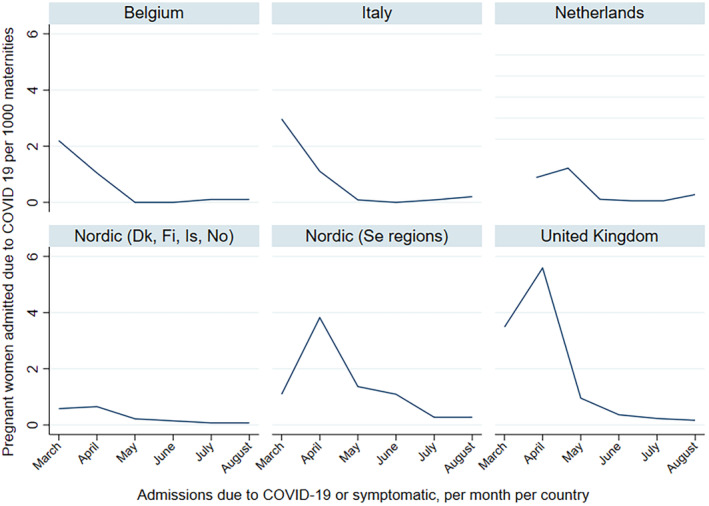
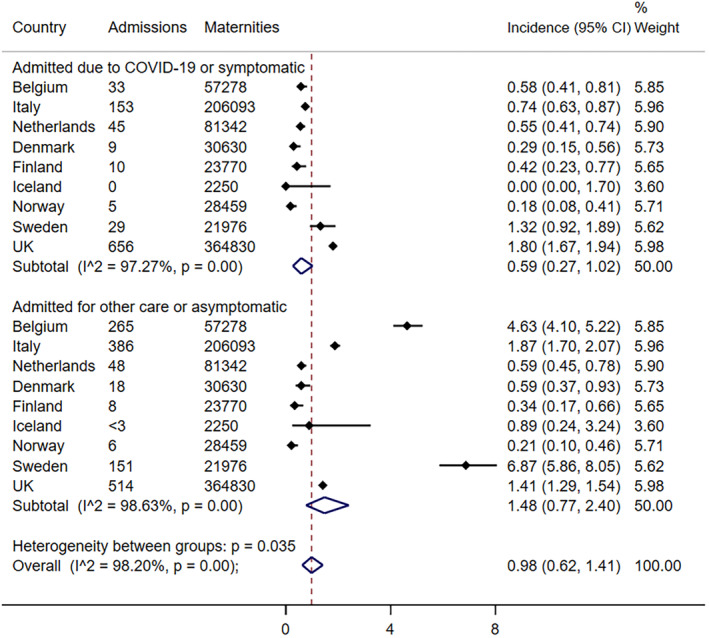
In a source population of 816 628 maternities, a total of 2338 pregnant women were admitted with SARS-CoV-2; among them 940 (40%) were COVID-19-related admissions. The pooled incidence estimate for COVID-19-related admission was 0.59 (95% confidence interval 0.27-1.02) per 1000 maternities, with notable heterogeneity across countries (I = 97.3%, P = 0.00). In the COVID-19 admission group, between 8% and 17% of the women were admitted to intensive care, and 5%-13% needed mechanical ventilation. Thromboprophylaxis was the most frequent treatment given during COVID-19-related admission (range 14%-55%). Among 908 infants born to women in the COVID-19-related admission group, 5 (0.6%) stillbirths were reported.
During the initial months of the pandemic, we found substantial variations in incidence of COVID-19-related admissions in nine European countries. Few pregnant women received COVID-19-directed medical treatment. Several barriers to rapid surveillance were identified. Investment in robust surveillance should be prioritized to prepare for future pandemics.
大多数关于妊娠合并 COVID-19 的数据并非来自健全的基于人群的主动监测系统。
我们在国际产科调查系统网络(INOSS)内使用标准化定义,对多国基于人群的国家或地区前瞻性队列进行了一项研究。在 2020 年 3 月 1 日至 8 月 31 日期间分娩的妇女源人群中,我们纳入了在住院前 7 天内或住院期间 SARS-CoV-2 PCR 检测阳性且住院时间不超过产后 2 天的孕妇。这些住院进一步分为 COVID-19 相关和非 COVID-19 相关。主要观察指标为 COVID-19 相关住院的发病率。次要结局包括严重产妇疾病(入住 ICU 和机械通气)和 COVID-19 针对性治疗。
在 816628 例产妇源人群中,共有 2338 例孕妇因 SARS-CoV-2 住院;其中 940 例(40%)为 COVID-19 相关住院。COVID-19 相关住院的汇总发病率估计值为每 1000 例产妇 0.59(95%置信区间 0.27-1.02),各国之间存在显著异质性(I ² = 97.3%,P = 0.00)。在 COVID-19 住院组中,8%-17%的妇女入住 ICU,5%-13%需要机械通气。COVID-19 相关住院期间最常给予的治疗是血栓预防(范围 14%-55%)。在 COVID-19 相关住院组的 908 例婴儿中,报告了 5 例(0.6%)死胎。
在大流行的最初几个月,我们发现 9 个欧洲国家 COVID-19 相关住院的发病率存在很大差异。很少有孕妇接受 COVID-19 针对性治疗。确定了一些快速监测的障碍。应优先投资建立健全的监测系统,为未来的大流行做好准备。