Clinical Haematology, Peter MacCallum Cancer Centre, Melbourne, Australia.
Clinical Haematology, Royal Melbourne Hospital, Parkville, Australia.
Blood. 2023 Nov 23;142(21):1784-1788. doi: 10.1182/blood.2023020158.
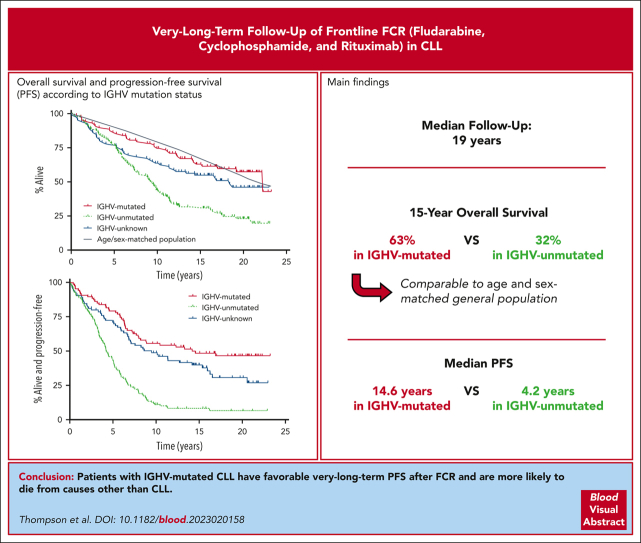
Chemoimmunotherapy with fludarabine, cyclophosphamide, and rituximab (FCR) achieves durable remissions, with flattening of the progression-free survival (PFS) curve in patients with mutated immunoglobulin heavy chain variable gene (IGHV-M). We updated long-term follow-up results from the original 300-patient FCR study initiated at MD Anderson in 1999. The current median follow-up is 19.0 years. With this extended follow-up, the median PFS for patients with IGHV-M was 14.6 years vs 4.2 years for patients with unmutated IGHV (IGHV-UM). Disease progression beyond 10 years was uncommon. In total, 16 of 94 (17%) patients in remission at 10 years subsequently progressed with the additional follow-up compared with the patients in our prior report in 2015. Only 4 of 45 patients (9%) with IGHV-M progressed beyond 10 years. Excluding Richter transformation, 96 of 300 patients (32%) developed 106 other malignancies, with 19 of 300 (6.3%) developing therapy-related myeloid neoplasms (tMNs), which were fatal in 16 of 19 (84%). No pretreatment patient characteristics predicted the risk of tMNs. In summary, FCR remains an option for patients with IGHV-M chronic lymphocytic leukemia (CLL), with a significant fraction achieving functional cure of CLL. A risk-benefit assessment is warranted when counseling patients, balancing potential functional cure with the risk of late relapses and serious secondary malignancies.
氟达拉滨、环磷酰胺和利妥昔单抗(FCR)联合化疗可使免疫球蛋白重链可变区(IGHV)发生突变的患者获得持久缓解,并使无进展生存期(PFS)曲线趋于平坦。我们更新了 1999 年在 MD 安德森癌症中心启动的最初 300 例 FCR 研究的长期随访结果。目前的中位随访时间为 19.0 年。通过这次延长随访,IGHV-M 患者的中位 PFS 为 14.6 年,而 IGHV 未突变(IGHV-UM)患者的中位 PFS 为 4.2 年。10 年以上的疾病进展并不常见。在缓解 10 年的 94 例患者中,有 16 例(17%)在额外随访中出现进展,与我们在 2015 年的报告中的患者相比有所增加。仅有 4 例(9%)IGHV-M 患者在 10 年以上出现进展。排除 Richter 转化,300 例患者中有 96 例(32%)发生了 106 种其他恶性肿瘤,其中 19 例(6.3%)发生了治疗相关髓系肿瘤(tMNs),19 例中的 16 例(84%)是致命的。没有患者特征可以预测 tMNs 的风险。总之,FCR 仍然是IGHV-M 慢性淋巴细胞白血病(CLL)患者的一种选择,有很大一部分患者可以实现 CLL 的功能性治愈。在为患者提供咨询时,需要权衡潜在的功能性治愈与晚期复发和严重继发性恶性肿瘤的风险,进行风险效益评估。