Department of Radiology, Funan County People's Hospital, Fuyang, Anhui, China.
Department of Radiology, The Affiliated Hospital of Nanjing University of Chinese Medicine, Nanjing, China.
Clin Transl Sci. 2023 Nov;16(11):2209-2221. doi: 10.1111/cts.13621. Epub 2023 Sep 5.
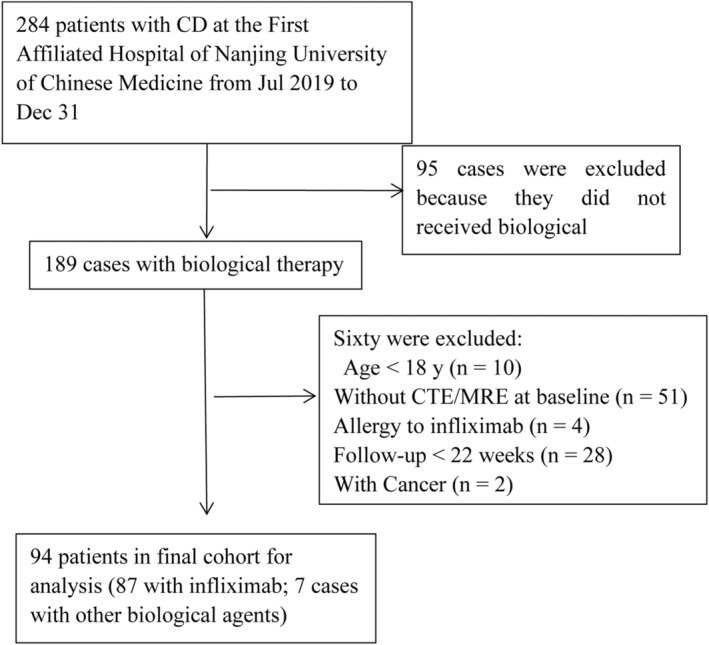
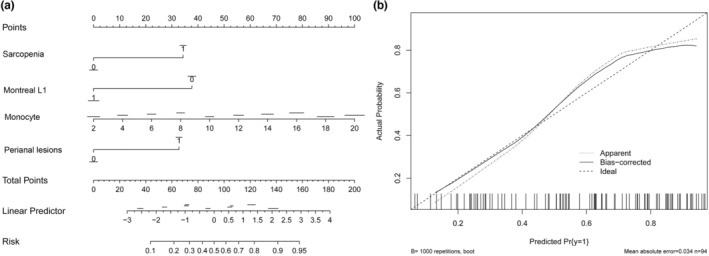
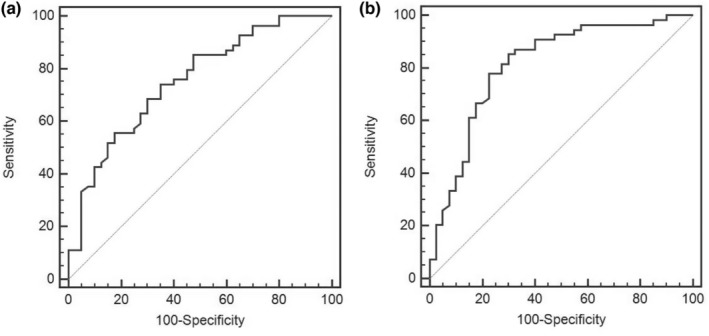
Sarcopenia occurs in patients with Crohn's disease (CD). However, the association between sarcopenia and loss of response (LOR) to biologic agents remains unclear. This study explored such an association in CD patients. This retrospective study included 94 CD patients who received biologic therapy. The skeletal muscle cross-sectional area at the third lumbar was assessed by computed tomography or magnetic resonance imaging for sarcopenia evaluation. A LOR was defined by fecal calprotectin (FC) < 250 μg/g or >50% reduction from baseline levels or other factors, such as the used agent being replaced by other biologic agents. The association between sarcopenia and LOR was assessed by logistic regression analysis. LOR was observed in 54 patients (57.4%). The prevalence of sarcopenia in the LOR group was higher than that in response group (70.4% vs. 40.0%, p = 0.003). Sarcopenia (odds ratio [OR] = 3.89, 95% confidence interval [CI]: 1.31-11.54), Montreal L1 type (OR = 0.20, 95% CI: 0.06-0.60), perianal lesions (OR = 4.08, 95% CI: 1.31-12.70), and monocytes percentage (OR = 1.27, 95% CI: 1.02-1.57) at baseline were independent associated factors for LOR. Sarcopenia was also associated with LOR in patients who received infliximab (OR = 3.31, 95% CI: 1.11-9.87). Montreal L1 type, perianal lesions, and monocytes percentage (Model 1), and with additional consideration of sarcopenia (Model 2), were developed to predict LOR. Model 2 showed better performance than Model 1 (area under the curve [AUC] 0.82 vs. 0.75). Sarcopenia was associated with the LOR to biological agents or infliximab in adult patients with CD.
肌肉减少症发生于克罗恩病(CD)患者中。然而,肌肉减少症与生物制剂应答丧失(LOR)之间的关系尚不清楚。本研究旨在探讨 CD 患者中这种关系。本回顾性研究纳入了 94 名接受生物治疗的 CD 患者。通过计算机断层扫描或磁共振成像评估第三腰椎的骨骼肌横截面积以评估肌肉减少症。LOR 定义为粪便钙卫蛋白(FC)<250μg/g 或较基线水平下降>50%,或其他因素,如所使用的药物被其他生物制剂替代。通过逻辑回归分析评估肌肉减少症与 LOR 之间的关系。54 名患者(57.4%)出现 LOR。在 LOR 组中,肌肉减少症的发生率高于应答组(70.4% vs. 40.0%,p=0.003)。肌肉减少症(比值比[OR] = 3.89,95%置信区间[CI]:1.31-11.54)、蒙特利尔 L1 型(OR = 0.20,95% CI:0.06-0.60)、肛周病变(OR = 4.08,95% CI:1.31-12.70)和基线时的单核细胞百分比(OR = 1.27,95% CI:1.02-1.57)是 LOR 的独立相关因素。在接受英夫利昔单抗治疗的患者中,肌肉减少症也与 LOR 相关(OR = 3.31,95% CI:1.11-9.87)。蒙特利尔 L1 型、肛周病变和单核细胞百分比(模型 1),以及在考虑到肌肉减少症后(模型 2),被开发用于预测 LOR。模型 2 的表现优于模型 1(曲线下面积[AUC]0.82 比 0.75)。肌肉减少症与成人 CD 患者对生物制剂或英夫利昔单抗的 LOR 相关。