Muddu Martin, Semitala Fred Collins, Kimera Isaac Derick, Musimbaggo Douglas Joseph, Mbuliro Mary, Ssennyonjo Rebecca, Kigozi Simon Peter, Katwesigye Rodgers, Ayebare Florence, Namugenyi Christabellah, Mugabe Frank, Mutungi Gerald, Longenecker Chris T, Katahoire Anne R, Schwartz Jeremy I, Ssinabulya Isaac
Makerere University Joint AIDS Program (MJAP), P.O. Box 7072, Kampala, Uganda.
Makerere University College of Health Sciences, Kampala, Uganda.
Implement Sci Commun. 2023 Aug 25;4(1):102. doi: 10.1186/s43058-023-00488-2.
World Health Organization (WHO) HEARTS packages are increasingly used to control hypertension. However, their feasibility in persons living with HIV (PLHIV) is unknown. We studied the effectiveness and implementation of a WHO HEARTS intervention to integrate the management of hypertension into HIV care.
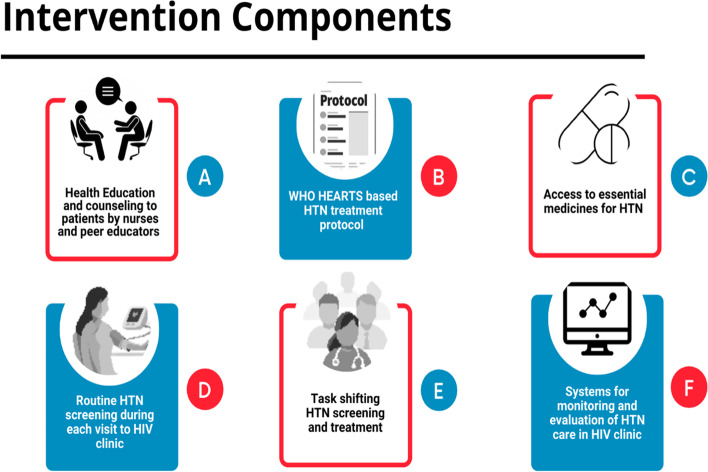
This was a mixed methods study at Uganda's largest HIV clinic. Components of the adapted WHO HEARTS intervention were lifestyle counseling, free hypertension medications, hypertension treatment protocol, task shifting, and monitoring tools. We determined the effectiveness of the intervention among PLHIV by comparing hypertension and HIV outcomes at baseline and 21 months. The RE-AIM framework was used to evaluate the implementation outcomes of the intervention at 21 months. We conducted four focus group discussions with PLHIV (n = 42), in-depth interviews with PLHIV (n = 9), healthcare providers (n = 15), and Ministry of Health (MoH) policymakers (n = 2).
Reach: Among the 15,953 adult PLHIV in the clinic, of whom 3892 (24%) had been diagnosed with hypertension, 1133(29%) initiated integrated hypertension-HIV treatment compared to 39 (1%) at baseline. Among the enrolled patients, the mean age was 51.5 ± 9.7 years and 679 (62.6%) were female.
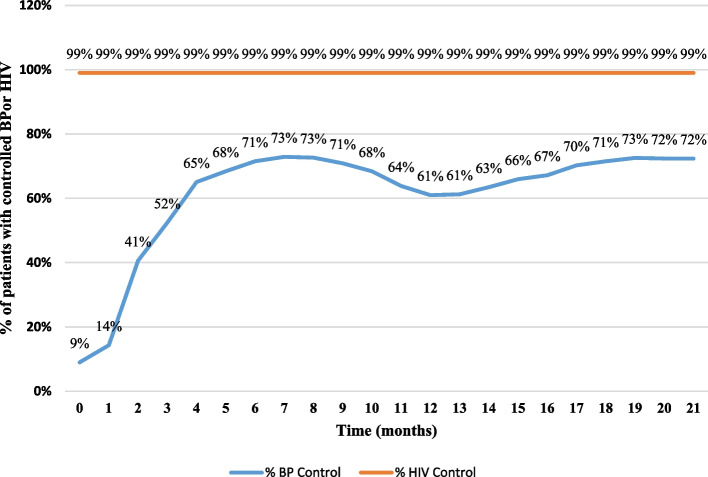
Among the treated patients, hypertension control improved from 9 to 72% (p < 0.001), mean systolic blood pressure (BP) from 153.2 ± 21.4 to 129.2 ± 15.2 mmHg (p < 0.001), and mean diastolic BP from 98.5 ± 13.5 to 85.1 ± 9.7 mmHg (p < 0.001). Overall, 1087 (95.9%) of patients were retained by month 21. HIV viral suppression remained high, 99.3 to 99.5% (p = 0.694). Patients who received integrated hypertension-HIV care felt healthy and saved more money. Adoption: All 48 (100%) healthcare providers in the clinic were trained and adopted the intervention. Training healthcare providers on WHO HEARTS, task shifting, and synchronizing clinic appointments for hypertension and HIV promoted adoption.
WHO HEARTS intervention was feasible and implemented with fidelity. Maintenance: Leveraging HIV program resources and adopting WHO HEARTS protocols into national guidelines will promote sustainability.
The WHO HEARTS intervention promoted the integration of hypertension management into HIV care in the real-world setting. It was acceptable, feasible, and effective in controlling hypertension and maintaining optimal viral suppression among PLHIV. Integrating this intervention into national guidelines will promote sustainability.
世界卫生组织(WHO)的HEARTS套餐越来越多地用于控制高血压。然而,其在艾滋病毒感染者(PLHIV)中的可行性尚不清楚。我们研究了WHO的HEARTS干预措施将高血压管理纳入艾滋病毒护理的有效性和实施情况。
这是一项在乌干达最大的艾滋病毒诊所进行的混合方法研究。经调整的WHO HEARTS干预措施的组成部分包括生活方式咨询、免费高血压药物、高血压治疗方案、任务转移和监测工具。我们通过比较基线和21个月时的高血压和艾滋病毒结果,确定了该干预措施在PLHIV中的有效性。采用RE-AIM框架评估21个月时干预措施的实施结果。我们与PLHIV(n = 42)进行了四次焦点小组讨论,对PLHIV(n = 9)、医疗服务提供者(n = 15)和卫生部(MoH)政策制定者(n = 2)进行了深入访谈。
覆盖范围:在该诊所的15953名成年PLHIV中,3892人(24%)被诊断患有高血压,1133人(29%)开始接受高血压-艾滋病毒综合治疗,而基线时为39人(1%)。在登记的患者中,平均年龄为51.5±9.7岁,679人(62.6%)为女性。
在接受治疗的患者中,高血压控制率从9%提高到72%(p < 0.001),平均收缩压(BP)从153.2±21.4 mmHg降至129.2±15.2 mmHg(p < 0.001),平均舒张压从98.5±13.5 mmHg降至85.1±9.7 mmHg(p < 0.001)。总体而言,到第21个月时,1087名(95.9%)患者仍在接受治疗。艾滋病毒病毒抑制率仍然很高,为99.3%至99.5%(p = 0.694)。接受高血压-艾滋病毒综合护理的患者感觉健康,节省了更多费用。采用:诊所的所有48名(100%)医疗服务提供者都接受了培训并采用了该干预措施。对医疗服务提供者进行WHO HEARTS、任务转移以及同步高血压和艾滋病毒诊所预约的培训促进了采用。
WHO HEARTS干预措施是可行的,并得到了忠实执行。维持:利用艾滋病毒项目资源并将WHO HEARTS方案纳入国家指南将促进可持续性。
WHO的HEARTS干预措施促进了在现实环境中将高血压管理纳入艾滋病毒护理。它在控制高血压和维持PLHIV的最佳病毒抑制方面是可接受的、可行的和有效的。将该干预措施纳入国家指南将促进可持续性。