Health and Social Surveys Group, Research Department of Epidemiology and Public Health, University College London (UCL), London, UK.
Aceso Global Health Consultants Pte Limited, Singapore, Singapore.
Eur J Public Health. 2023 Dec 9;33(6):959-967. doi: 10.1093/eurpub/ckad146.
Social-economic factors and health behaviours may be driving variation in ethnic health inequalities in multimorbidity including among distinct ethnic groups.
Using the cross-sectional nationally representative Health Surveys for England 2011-18 (N = 54 438, aged 16+), we performed multivariable logistic regression on the odds of having general multimorbidity (≥2 longstanding conditions) by ethnicity [British White (reference group), White Irish, Other White, Indian, Pakistani, Bangladeshi, Chinese, African, Caribbean, White mixed, Other Mixed], adjusting for age, sex, education, area deprivation, obesity, smoking status and survey year. This was repeated for cardiovascular multimorbidity (N = 37 148, aged 40+: having ≥2 of the following: self-reported diabetes, hypertension, heart attack or stroke) and multiple cardiometabolic risk biomarkers (HbA1c ≥6.5%, raised blood pressure, total cholesterol ≥5mmol/L).
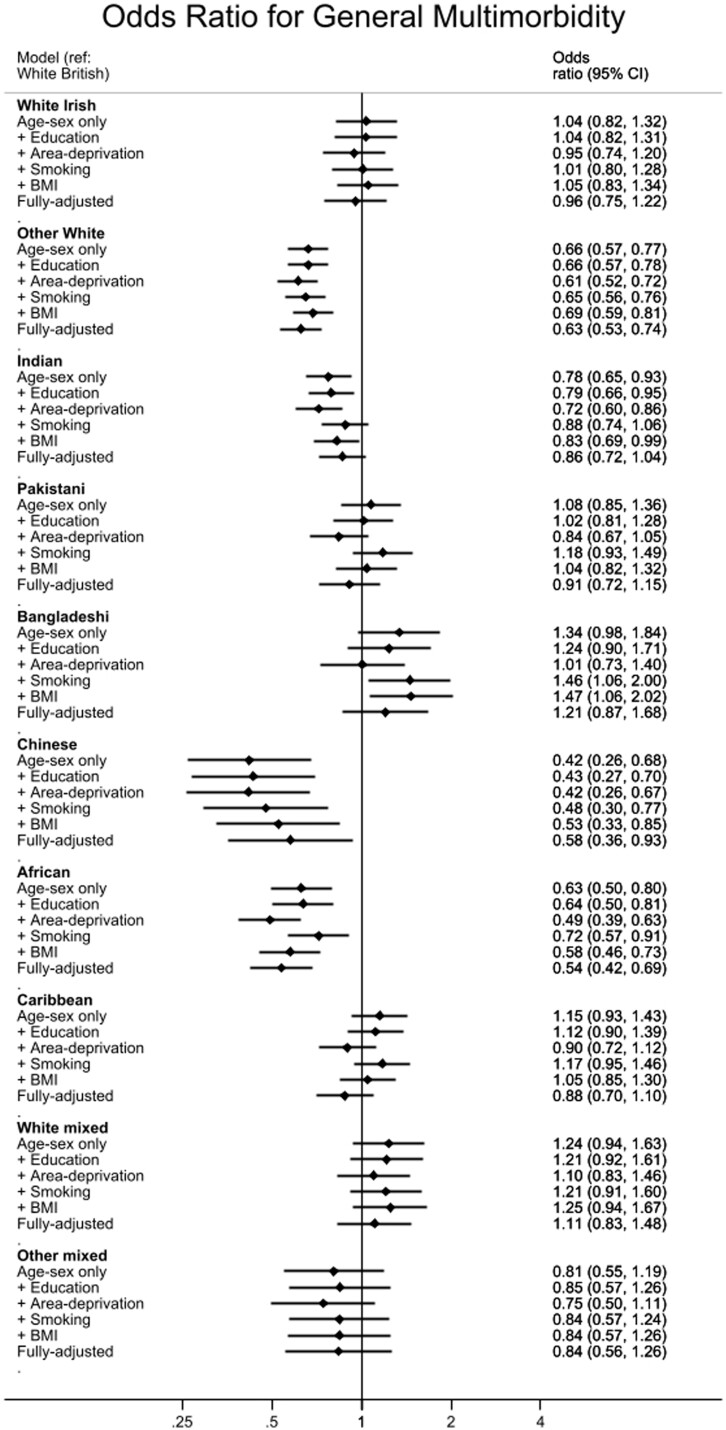
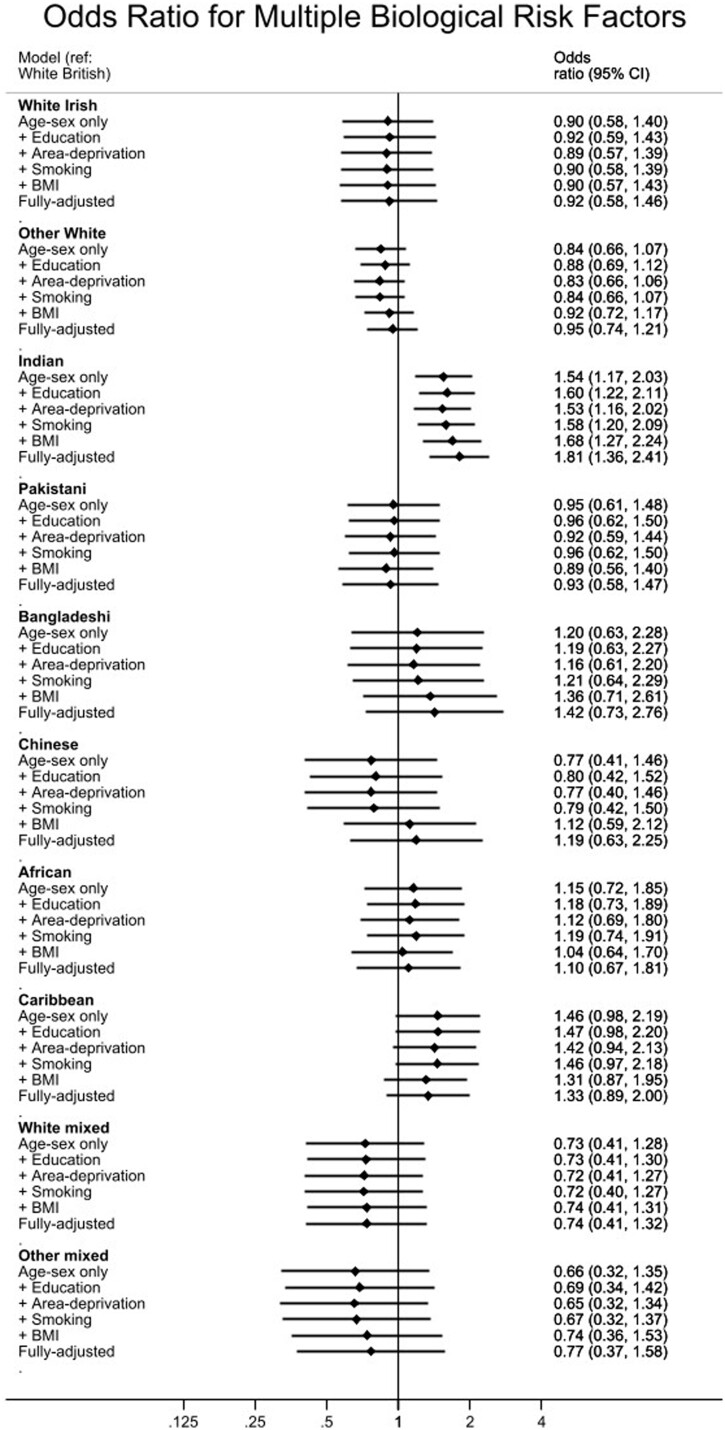
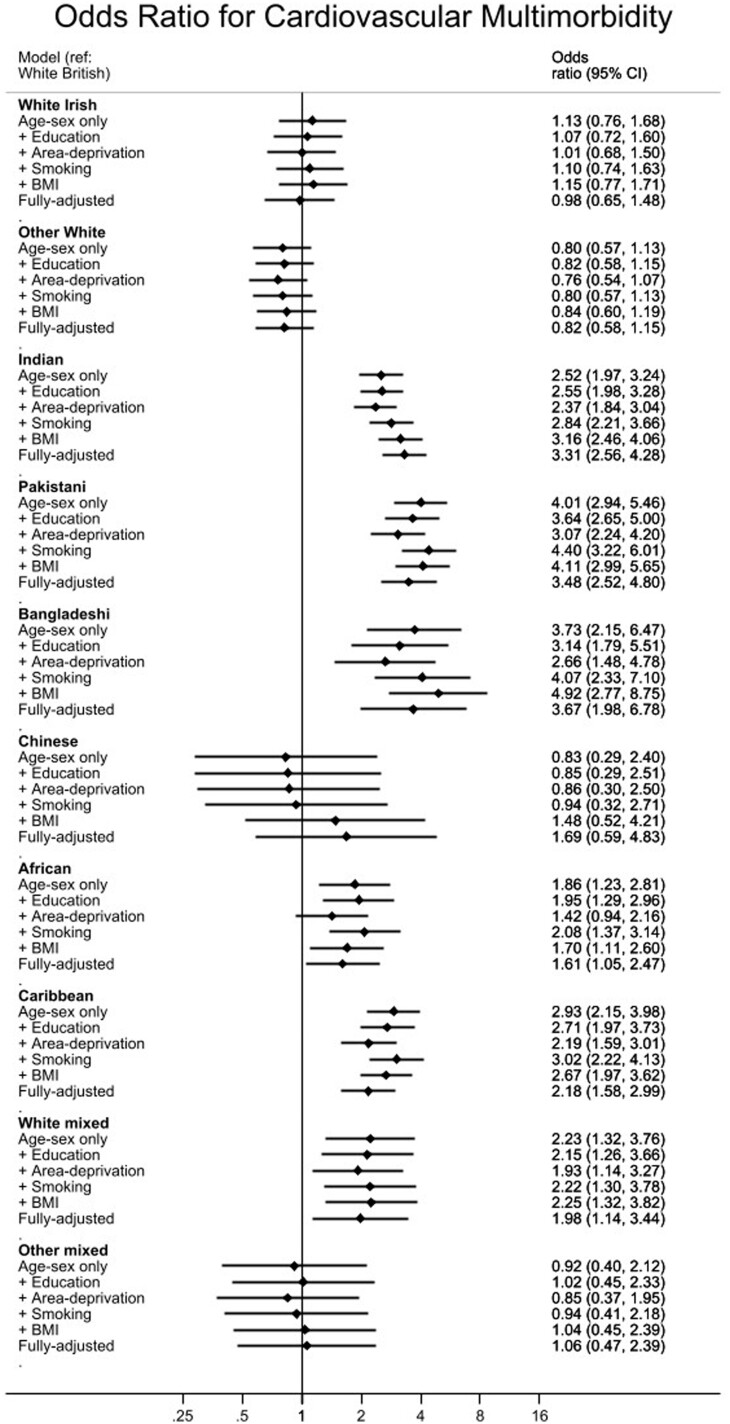
Twenty percent of adults had general multimorbidity. In fully adjusted models, compared with the White British majority, Other White [odds ratio (OR) = 0.63; 95% confidence interval (CI) 0.53-0.74], Chinese (OR = 0.58, 95% CI 0.36-0.93) and African adults (OR = 0.54, 95% CI 0.42-0.69), had lower odds of general multimorbidity. Among adults aged 40+, Pakistani (OR = 1.27, 95% CI 0.97-1.66; P = 0.080) and Bangladeshi (OR = 1.75, 95% CI 1.16-2.65) had increased odds, and African adults had decreased odds (OR = 0.63, 95% CI 0.47-0.83) of general multimorbidity. Risk of cardiovascular multimorbidity was higher among Indian (OR = 3.31, 95% CI 2.56-4.28), Pakistani (OR = 3.48, 95% CI 2.52-4.80), Bangladeshi (OR = 3.67, 95% CI 1.98-6.78), African (OR = 1.61, 95% CI 1.05-2.47), Caribbean (OR = 2.18, 95% CI 1.59-2.99) and White mixed (OR = 1.98, 95% CI 1.14-3.44) adults. Indian adults were also at risk of having multiple cardiometabolic risk biomarkers.
Ethnic inequalities in multimorbidity are independent of social-economic factors. Ethnic minority groups are particularly at risk of cardiovascular multimorbidity, which may be exacerbated by poorer management of cardiometabolic risk requiring further investigation.
社会经济因素和健康行为可能是导致多种疾病中种族健康不平等的原因,包括不同种族群体之间。
我们使用了 2011-2018 年全国代表性健康调查的横断面数据(N=54438 人,年龄在 16 岁及以上),根据种族(英国白人(参照组)、白爱尔兰人、其他白人、印度人、巴基斯坦人、孟加拉国人、中国人、非洲人、加勒比人、白人混合族裔、其他混合族裔),对多种合并症(≥2 种长期疾病)的发生几率进行了多变量逻辑回归分析,并调整了年龄、性别、教育程度、地区贫困程度、肥胖、吸烟状况和调查年份。对于心血管合并症(N=37148 人,年龄在 40 岁及以上:患有≥2 种以下疾病:自我报告的糖尿病、高血压、心脏病发作或中风)和多种心血管代谢风险生物标志物(HbA1c≥6.5%、血压升高、总胆固醇≥5mmol/L),我们重复了这一分析。
20%的成年人患有多种合并症。在完全调整的模型中,与白人英国多数族裔相比,其他白人(比值比(OR)=0.63;95%置信区间(CI)0.53-0.74)、中国人(OR=0.58,95%CI 0.36-0.93)和非洲裔成年人(OR=0.54,95%CI 0.42-0.69)患多种合并症的几率较低。在年龄在 40 岁及以上的成年人中,巴基斯坦人(OR=1.27,95%CI 0.97-1.66;P=0.080)和孟加拉国人(OR=1.75,95%CI 1.16-2.65)患多种合并症的几率增加,而非洲裔成年人患多种合并症的几率降低(OR=0.63,95%CI 0.47-0.83)。印度人(OR=3.31,95%CI 2.56-4.28)、巴基斯坦人(OR=3.48,95%CI 2.52-4.80)、孟加拉国人(OR=3.67,95%CI 1.98-6.78)、非洲人(OR=1.61,95%CI 1.05-2.47)、加勒比人(OR=2.18,95%CI 1.59-2.99)和白人混合族裔(OR=1.98,95%CI 1.14-3.44)成年人患心血管合并症的风险较高。印度成年人也存在多种心血管代谢风险生物标志物的风险。
多种合并症中的种族不平等独立于社会经济因素。少数民族群体尤其面临心血管多种合并症的风险,这可能由于对心血管代谢风险的管理不善而加剧,需要进一步调查。