Malcolm Rebecca J, Pilkington Mercedes, Merchant Shaila J, Velez Maria P, Brogly Susan B
From the Department of Biomedical Sciences, Queen's University, Kingston, Canada.
Division of Pediatric Surgery, University of Calgary, Calgary, Canada.
Ann Surg Open. 2021 May 19;2(2):e069. doi: 10.1097/AS9.0000000000000069. eCollection 2021 Jun.
To describe work-related factors, pregnancy, and pregnancy outcomes in female surgeons is the objective of this study.
Some data suggest surgeon workload may deter pregnancy and adversely affect pregnancy outcomes in female surgeons.
A cross-sectional, web-based survey was distributed via e-mail to members of the Society of Obstetrics and Gynaecologists of Canada and to surgical departments of 6 Canadian universities from October 2019 to January 2020.
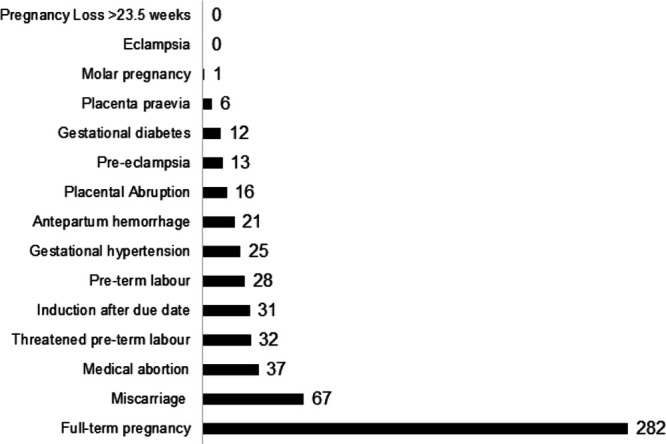
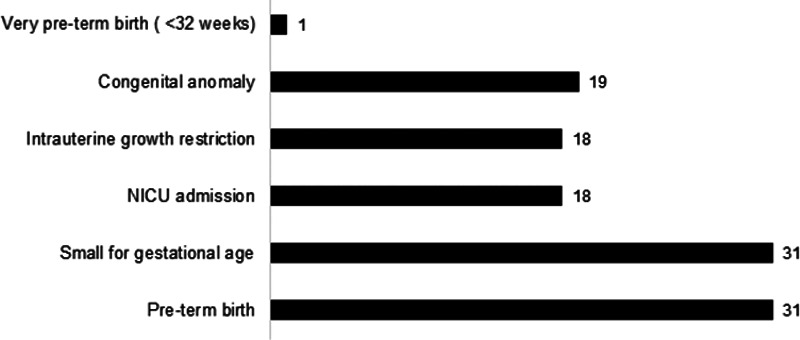
A total of 223 surgeons with 451 pregnancies participated. Work hours were reduced in 33.3% of pregnancies, and 28.0% had a policy for pregnancy in their workplace. A total of 57% of surgeons intentionally delayed pregnancy due to heavy workload and 39% to career concerns, and 31% reported work adversely affected their pregnancy. Adverse maternal outcomes included miscarriage (14.9%), preterm labor (6.2%), hypertension (5.5%), pre-eclampsia (2.9%), and placenta praevia (1.3%). Adverse infant outcomes included preterm birth (6.9%), small for gestational age at birth (6.9%), and neonatal intensive care unit admission (4%). Congenital anomalies occurred in 4.2% of pregnancies. Surgeons who reported a policy for working while pregnant were more likely to have reduced their work hours than those without a policy (48.4% vs 28.5% respectively, < 0.0001). In unadjusted models, those who reduced their work hours while pregnant were less likely to have a miscarriage than those who did not (odds ratio = 0.2, 95% confidence interval, 0.1-0.4).
Female surgeons reported delays in pregnancy due to work, adverse effects of work on pregnancy, and some elevated rates of adverse outcomes. These data support policies for pregnancy in surgeons and surgical trainees.
本研究的目的是描述女外科医生的工作相关因素、妊娠情况及妊娠结局。
一些数据表明,外科医生的工作量可能会阻碍妊娠,并对女外科医生的妊娠结局产生不利影响。
2019年10月至2020年1月,通过电子邮件向加拿大妇产科学会会员以及加拿大6所大学的外科部门发放了一项基于网络的横断面调查问卷。
共有223名外科医生参与了451次妊娠。33.3%的妊娠期间工作时间减少,28.0%的工作场所制定了妊娠相关政策。共有57%的外科医生因工作量大而有意推迟妊娠,39%因职业担忧而推迟,31%报告工作对其妊娠产生了不利影响。不良孕产妇结局包括流产(14.9%)、早产(6.2%)、高血压(5.5%)、先兆子痫(2.9%)和前置胎盘(1.3%)。不良婴儿结局包括早产(6.9%)、出生时小于胎龄(6.9%)和新生儿重症监护病房入院(4%)。4.2%的妊娠出现先天性异常。报告有孕期工作政策的外科医生比没有该政策的医生更有可能减少工作时间(分别为48.4%和28.5%,<0.0001)。在未调整的模型中,孕期减少工作时间的医生流产的可能性低于未减少工作时间的医生(比值比=0.2,95%置信区间,0.1 - 0.4)。
女外科医生报告因工作导致妊娠推迟、工作对妊娠产生不利影响以及一些不良结局发生率有所升高。这些数据支持为外科医生和外科实习生制定妊娠相关政策。