Department of Neurology, AG Emergency and Critical Care Neurology, Campus Virchow-Klinikum, Charité Universitätsmedizin Berlin, Augustenburger Platz 1, 13353, Berlin, Germany.
Department of Clinical Sciences Lund, Clinical Neurophysiology, Lund University, Skane University Hospital, Getingevägen 4, 22185, Lund, Sweden.
J Neurol. 2023 Dec;270(12):5999-6009. doi: 10.1007/s00415-023-11951-4. Epub 2023 Aug 28.
Bilaterally absent cortical somatosensory evoked potentials (SSEPs) reliably predict poor outcome in comatose cardiac arrest (CA) patients. Cortical SSEP amplitudes are a recent prognostic extension; however, amplitude thresholds, inter-recording, and inter-rater agreement remain uncertain.
In a retrospective multicenter cohort study, we determined cortical SSEP amplitudes of comatose CA patients using a standardized evaluation pathway. We studied inter-recording agreement in repeated SSEPs and inter-rater agreement by four raters independently determining 100 cortical SSEP amplitudes. Primary outcome was assessed using the cerebral performance category (CPC) upon intensive care unit discharge dichotomized into good (CPC 1-3) and poor outcome (CPC 4-5).
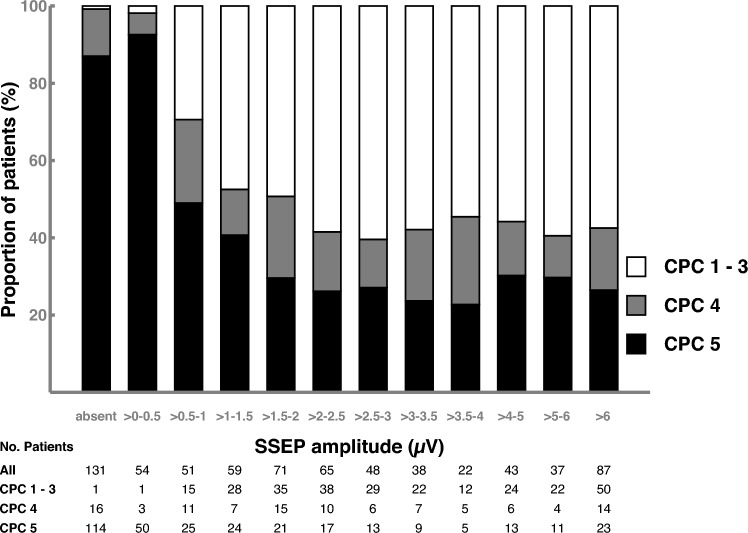
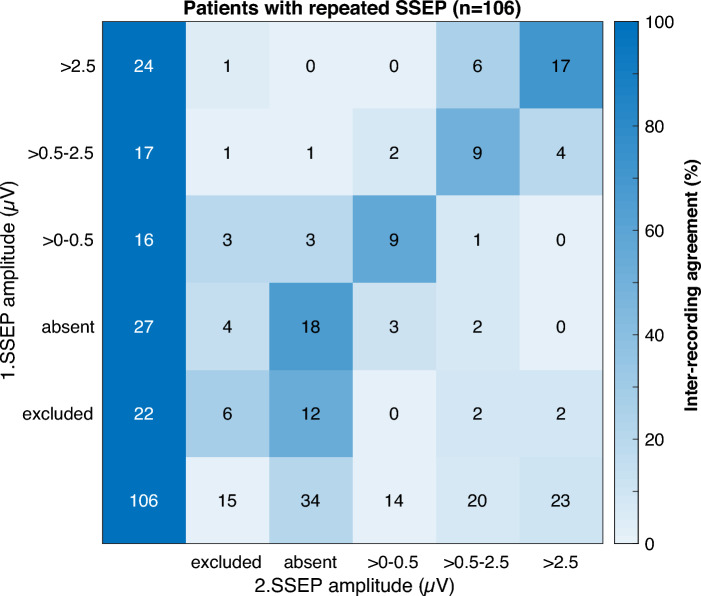
Of 706 patients with SSEPs with median 3 days after CA, 277 (39.2%) had good and 429 (60.8%) poor outcome. Of patients with bilaterally absent cortical SSEPs, one (0.8%) survived with CPC 3 and 130 (99.2%) had poor outcome. Otherwise, the lowest cortical SSEP amplitude in good outcome patients was 0.5 µV. 184 (42.9%) of 429 poor outcome patients had lower cortical SSEP amplitudes. In 106 repeated SSEPs, there were 6 (5.7%) with prognostication-relevant changes in SSEP categories. Following a standardized evaluation pathway, inter-rater agreement was almost perfect with a Fleiss' kappa of 0.88.
Bilaterally absent and cortical SSEP amplitudes below 0.5 µV predicted poor outcome with high specificity. A standardized evaluation pathway provided high inter-rater and inter-recording agreement. Regain of consciousness in patients with bilaterally absent cortical SSEPs rarely occurs. High-amplitude cortical SSEP amplitudes likely indicate the absence of severe brain injury.
双侧皮质体感诱发电位(SSEP)缺失可靠地预测昏迷性心脏骤停(CA)患者的不良预后。皮质 SSEP 幅度是最近的预后扩展;然而,幅度阈值、记录间和评分者间的一致性仍不确定。
在一项回顾性多中心队列研究中,我们使用标准化评估途径确定昏迷性 CA 患者的皮质 SSEP 幅度。我们研究了重复 SSEPs 的记录间一致性和四位评分者独立确定 100 个皮质 SSEP 幅度的评分者间一致性。主要结局是根据重症监护病房出院时的脑功能分类(CPC)评估,分为良好(CPC 1-3)和不良结局(CPC 4-5)。
在 706 例有 SSEP 的患者中,中位时间为 CA 后 3 天,277 例(39.2%)有良好结局,429 例(60.8%)有不良结局。双侧皮质 SSEP 缺失的患者中,有 1 例(0.8%)存活,CPC 为 3,130 例(99.2%)预后不良。否则,良好结局患者的皮质 SSEP 最低幅度为 0.5µV。429 例预后不良的患者中,有 184 例(42.9%)皮质 SSEP 幅度较低。在 106 次重复 SSEPs 中,有 6 次(5.7%)出现 SSEP 分类的预后相关变化。按照标准化评估途径,评分者间的一致性几乎是完美的,Fleiss'kappa 值为 0.88。
双侧缺失和皮质 SSEP 幅度低于 0.5µV 预测不良预后的特异性很高。标准化评估途径提供了高度的评分者间和记录间一致性。双侧皮质 SSEP 缺失的患者意识恢复很少发生。高幅度的皮质 SSEP 幅度可能表明不存在严重的脑损伤。