Lyme Disease Research Center, Division of Rheumatology, Department of Medicine, Johns Hopkins University School of Medicine, Baltimore, MD, USA.
Johns Hopkins HealthCare LLC, Glen Burnie, MD, USA.
BMC Health Serv Res. 2023 Aug 29;23(1):919. doi: 10.1186/s12913-023-09909-3.
Insurance claims data have been used to inform an understanding of Lyme disease epidemiology and cost of care, however few such studies have incorporated post-treatment symptoms following diagnosis. Using longitudinal data from a private, employer-based health plan in an endemic US state, we compared outpatient care utilization pre- and post-Lyme disease diagnosis. We hypothesized that utilization would be higher in the post-diagnosis period, and that temporal trends would differ by age and gender.
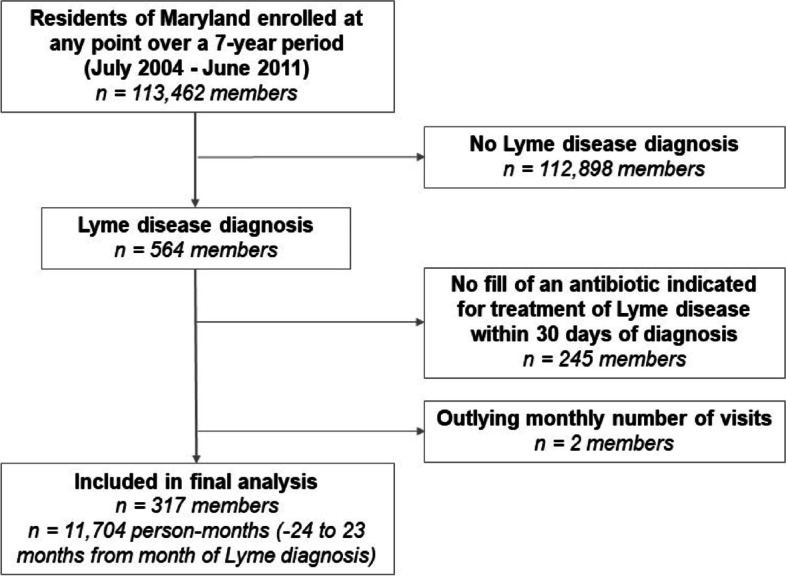
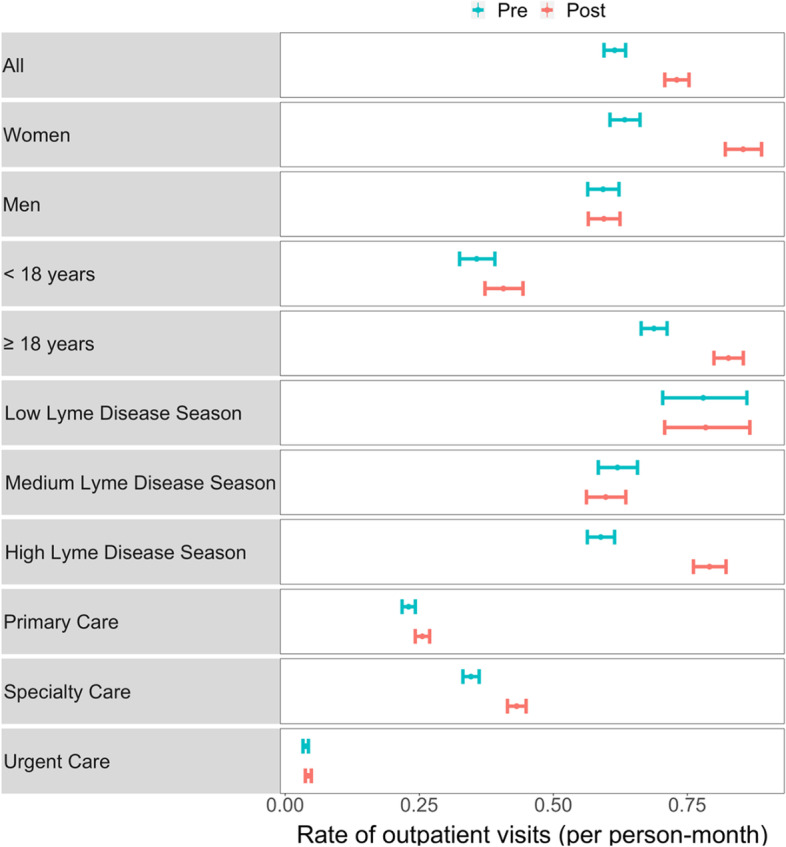
Members with Lyme disease were required to have both a corresponding ICD-9 code and a fill of an antibiotic indicated for treatment of the infection within 30 days of diagnosis. A 2-year 'pre- diagnosis' period and a 2-year 'post-diagnosis period' were centered around the diagnosis month. Lyme disease-relevant outpatient care visits were defined as specific primary care, specialty care, or urgent care visits. Descriptive statistics examined visits during these pre- and post-diagnosis periods, and the association between these periods and the number of visits was explored using generalized linear mixed effects models adjusting for age, season of the year, and gender.
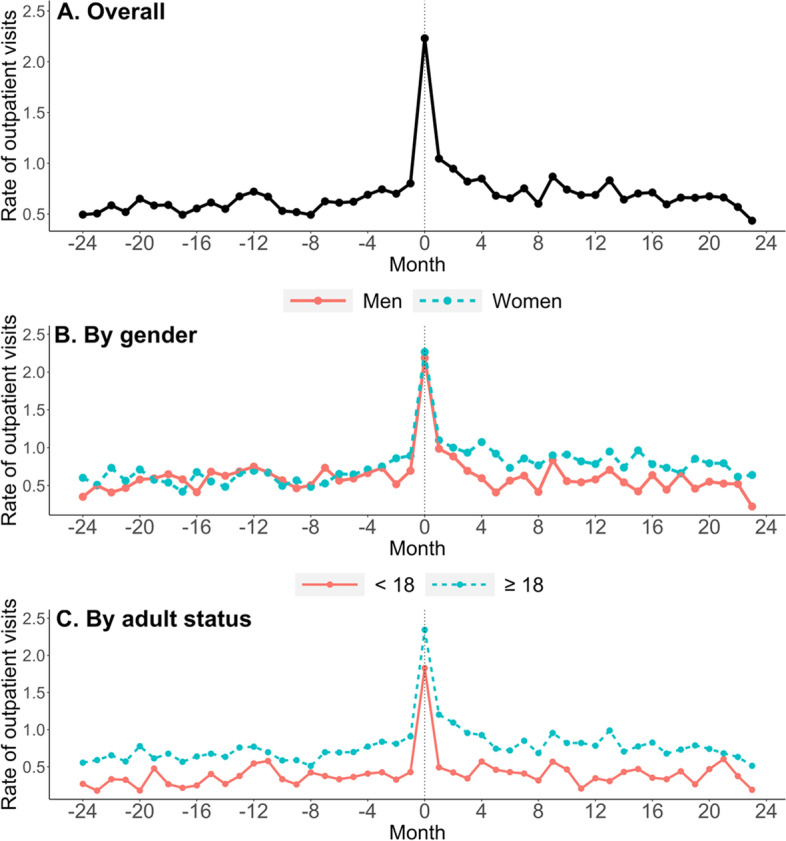
The rate of outpatient visits increased 26% from the pre to the post-Lyme disease diagnosis periods among our 317-member sample (rate ratio = 1.26 [1.18, 1.36], p < 0.001). Descriptively, care utilization increases appeared to persist across months in the post-diagnosis period. Women's care utilization increased by 36% (1.36 [1.24, 1.50], p < 0.001), a significantly higher increase than the 14% increase found among men (1.14 [1.02, 1.27], p = 0.017). This gender difference was mainly driven by adult members. We found a borderline significant 17% increase in visits for children < 18 years, (1.17 [0.99, 1.38], p = 0.068), and a 31% increase for adults ≥ 18 years (1.31 [1.21, 1.42], p < 0.001).
Although modest at the population level, the statistically significant increases in post-Lyme diagnosis outpatient care we observed were persistent and unevenly distributed across demographic and place of service categories. As Lyme disease cases continue to grow, so will the cumulative prevalence of persistent symptoms after treatment. Therefore, it will be important to confirm these findings and understand their significance for care utilization and cost, particularly against the backdrop of other post-acute infectious syndromes.
保险索赔数据已被用于了解莱姆病的流行病学和治疗费用,但很少有此类研究纳入诊断后治疗后的症状。本研究利用美国一个流行地区私人雇主健康计划的纵向数据,比较了莱姆病诊断前后的门诊护理利用情况。我们假设,在诊断后时期,利用会更高,并且时间趋势会因年龄和性别而异。
要求患有莱姆病的患者在诊断后 30 天内必须同时具有相应的 ICD-9 代码和抗生素的配药,以表明其接受了治疗感染的治疗。以诊断月份为中心,设定了为期 2 年的“诊断前”期和为期 2 年的“诊断后”期。莱姆病相关的门诊护理就诊被定义为特定的初级保健、专科保健或紧急护理就诊。描述性统计分析了这些诊断前和诊断后时期的就诊情况,并使用广义线性混合效应模型对年龄、季节和性别进行调整,探讨了这些时期与就诊次数之间的关联。
在我们的 317 名样本中,从莱姆病诊断前到诊断后的门诊就诊率增加了 26%(比率比=1.26 [1.18, 1.36],p<0.001)。从描述性分析来看,在诊断后时期,护理利用率的增加似乎持续存在于多个月份。女性的护理利用率增加了 36%(1.36 [1.24, 1.50],p<0.001),这一增长率明显高于男性的 14%(1.14 [1.02, 1.27],p=0.017)。这种性别差异主要是由成年成员驱动的。我们发现,18 岁以下儿童的就诊率增加了 17%(1.17 [0.99, 1.38],p=0.068),18 岁以上成年人的就诊率增加了 31%(1.31 [1.21, 1.42],p<0.001),这一结果具有边缘显著性。
尽管在人群水平上幅度较小,但我们观察到的莱姆病诊断后门诊护理利用率的显著增加是持续存在的,并且在人口统计学和服务场所类别之间分布不均。随着莱姆病病例的持续增加,治疗后持续存在症状的累积患病率也将增加。因此,确认这些发现并了解其对护理利用率和成本的意义非常重要,特别是在其他急性后感染综合征的背景下。