Section of Neurosurgery, Department of Medical Sciences, Uppsala University, 751 85, Uppsala, Sweden.
Brain Physics Laboratory, Division of Neurosurgery, Department of Clinical Neurosciences, University of Cambridge, Cambridge, UK.
Crit Care. 2023 Aug 31;27(1):339. doi: 10.1186/s13054-023-04627-y.
The primary aim was to explore the association of global cerebral physiological variables including intracranial pressure (ICP), cerebrovascular reactivity (PRx), cerebral perfusion pressure (CPP), and deviation from the PRx-based optimal CPP value (∆CPPopt; actual CPP-CPPopt) in relation to brain tissue oxygenation (pbtO) in traumatic brain injury (TBI).
A total of 425 TBI patients with ICP- and pbtO monitoring for at least 12 h, who had been treated at the neurocritical care unit, Addenbrooke's Hospital, Cambridge, UK, between 2002 and 2022 were included. Generalized additive models (GAMs) and linear mixed effect models were used to explore the association of ICP, PRx, CPP, and CPPopt in relation to pbtO. PbtO < 20 mmHg, ICP > 20 mmHg, PRx > 0.30, CPP < 60 mmHg, and ∆CPPopt < - 5 mmHg were considered as cerebral insults.
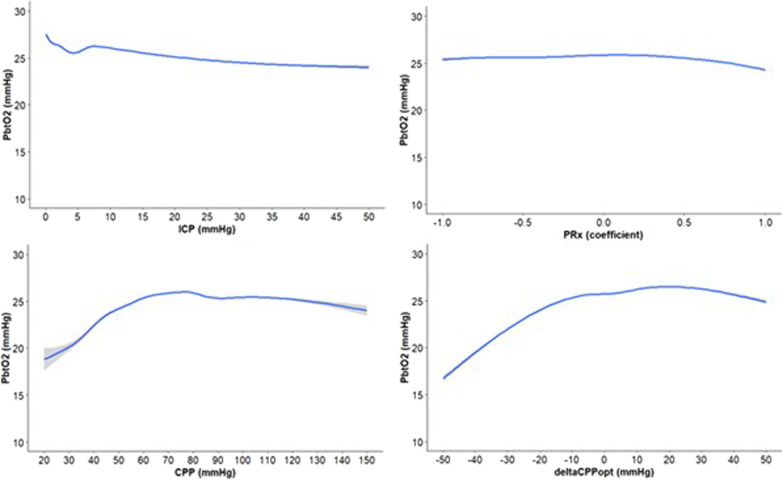
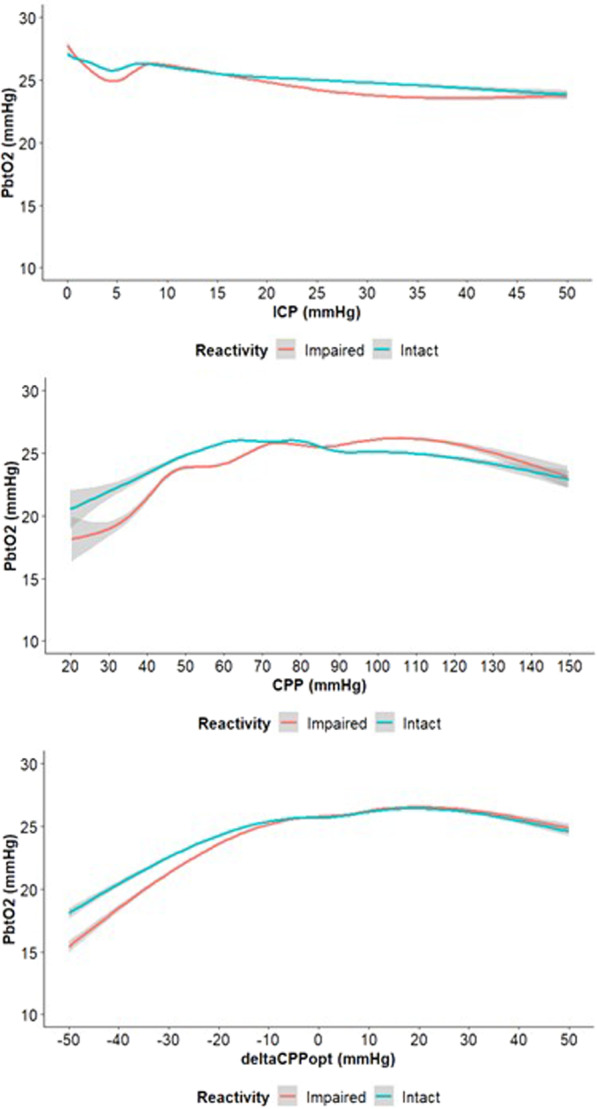
PbtO < 20 mmHg occurred in median during 17% of the monitoring time and in less than 5% in combination with ICP > 20 mmHg, PRx > 0.30, CPP < 60 mmHg, or ∆CPPopt < - 5 mmHg. In GAM analyses, pbtO remained around 25 mmHg over a large range of ICP ([0;50] mmHg) and PRx [- 1;1], but deteriorated below 20 mmHg for extremely low CPP below 30 mmHg and ∆CPPopt below - 30 mmHg. In linear mixed effect models, ICP, CPP, PRx, and ∆CPPopt were significantly associated with pbtO, but the fixed effects could only explain a very small extent of the pbtO variation.
PbtO below 20 mmHg was relatively frequent and often occurred in the absence of disturbances in ICP, PRx, CPP, and ∆CPPopt. There were significant, but weak associations between the global cerebral physiological variables and pbtO, suggesting that hypoxic pbtO is often a complex and independent pathophysiological event. Thus, other variables may be more crucial to explain pbtO and, likewise, pbtO may not be a suitable outcome measure to determine whether global cerebral blood flow optimization such as CPPopt therapy is successful.
本研究的主要目的是探讨颅内压(ICP)、脑血管反应性(PRx)、脑灌注压(CPP)和偏离基于 PRx 的最佳 CPP 值(∆CPPopt;实际 CPP-CPPopt)等全局脑生理变量与创伤性脑损伤(TBI)患者脑组织氧合(pbtO)之间的关系。
本研究纳入了 2002 年至 2022 年期间在英国剑桥阿登布鲁克医院神经重症监护病房接受 ICP 和 pbtO 监测至少 12 小时的 425 例 TBI 患者。使用广义加性模型(GAMs)和线性混合效应模型来探讨 ICP、PRx、CPP 和 CPPopt 与 pbtO 的关系。将 pbtO<20mmHg、ICP>20mmHg、PRx>0.30、CPP<60mmHg 和 ∆CPPopt<-5mmHg 视为脑损伤。
在监测期间的 17%时间内,pbtO<20mmHg 的中位数发生,在不到 5%的时间内与 ICP>20mmHg、PRx>0.30、CPP<60mmHg 或 ∆CPPopt<-5mmHg 同时发生。在 GAM 分析中,在较大的 ICP 范围([0;50]mmHg)和 PRx[-1;1]范围内,pbtO 仍保持在 25mmHg 左右,但当 CPP 极低(低于 30mmHg)和 ∆CPPopt 极低(低于-30mmHg)时,pbtO 会恶化至 20mmHg 以下。在线性混合效应模型中,ICP、CPP、PRx 和 ∆CPPopt 与 pbtO 显著相关,但固定效应只能解释 pbtO 变化的很小一部分。
pbtO<20mmHg 相对常见,且常发生于 ICP、PRx、CPP 和 ∆CPPopt 无波动时。全局脑生理变量与 pbtO 之间存在显著但较弱的关联,提示缺氧性 pbtO 通常是一种复杂的独立病理生理事件。因此,其他变量可能对解释 pbtO 更为重要,同样,pbtO 可能不是一个合适的结果测量指标,无法确定 CPPopt 治疗等是否成功优化了全局脑血流。