Secreto Carolina, Chean Dara, van de Louw Andry, Kouatchet Achille, Bauer Philippe, Cerrano Marco, Lengliné Etienne, Saillard Colombe, Chow-Chine Laurent, Perner Anders, Pickkers Peter, Soares Marcio, Rello Jordi, Pène Frédéric, Lemiale Virginie, Darmon Michael, Fodil Sofiane, Martin-Loeches Ignacio, Mehta Sangeeta, Schellongowski Peter, Azoulay Elie, Mokart Djamel
Division of Haematology, Department of Oncology, A.O.U. Città Della Salute e della Scienza di Torino, Turin, Italy.
Réanimation Polyvalente et Département d'Anesthésie et de Réanimation, Institut Paoli-Calmettes, Marseille, France.
Ann Intensive Care. 2023 Sep 2;13(1):79. doi: 10.1186/s13613-023-01172-3.
Acute respiratory failure (ARF) is the leading cause of intensive care unit (ICU) admission in patients with Acute Myeloid Leukemia (AML) and data on prognostic factors affecting short-term outcome are needed.
This is a post-hoc analysis of a multicenter, international prospective cohort study on immunocompromised patients with ARF admitted to ICU. We evaluated hospital mortality and associated risk factors in patients with AML and ARF; secondly, we aimed to define specific subgroups within our study population through a cluster analysis.
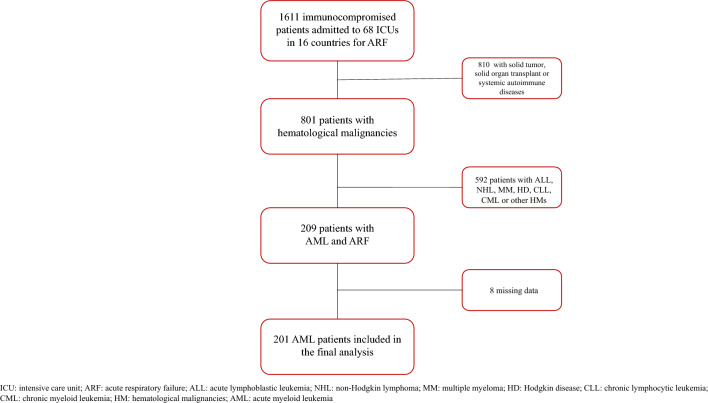
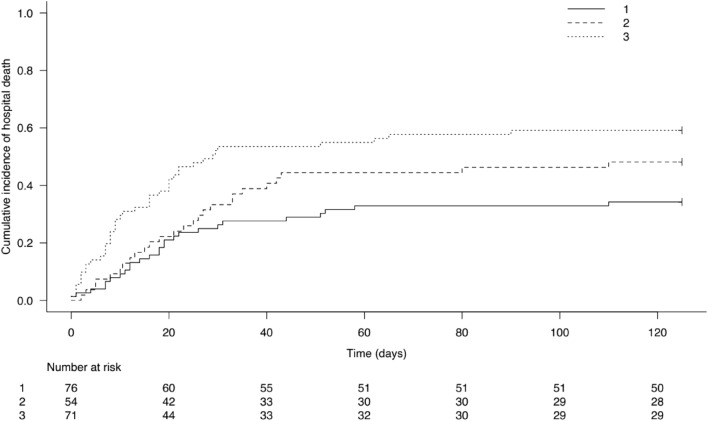
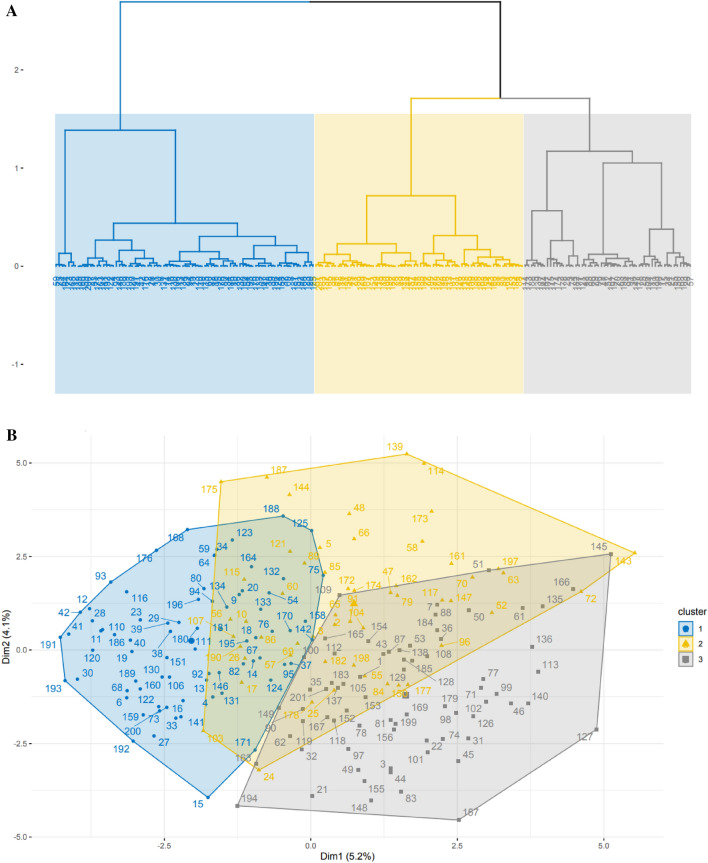
Overall, 201 of 1611 immunocompromised patients with ARF had AML and were included in the analysis. Hospital mortality was 46.8%. Variables independently associated with mortality were ECOG performance status ≥ 2 (OR = 2.79, p = 0.04), cough (OR = 2.94, p = 0.034), use of vasopressors (OR = 2.79, p = 0.044), leukemia-specific pulmonary involvement [namely leukostasis, pulmonary infiltration by blasts or acute lysis pneumopathy (OR = 4.76, p = 0.011)] and liver SOFA score (OR = 1.85, p = 0.014). Focal alveolar chest X-ray pattern was associated with survival (OR = 0.13, p = 0.001). We identified 3 clusters, that we named on the basis of the most frequently clinical, biological and radiological features found in each cluster: a "leukemic cluster", with high-risk AML patients with isolated, milder ARF; a "pulmonary cluster", consisting of symptomatic, highly oxygen-requiring, severe ARF with diffuse radiological findings in heavily immunocompromised patients; a clinical "inflammatory cluster", including patients with multi-organ failures in addition to ARF. When included in the multivariate analysis, cluster 2 and 3 were independently associated with hospital mortality.
Among AML patients with ARF, factors associated with a worse outcome are related to patient's background (performance status, leukemic pulmonary involvement), symptoms, radiological findings, the need for vasopressors and the liver SOFA score. We identified three specific ARF syndromes in AML patients, which showed a prognostic significance and could guide clinicians to optimize management strategies.
急性呼吸衰竭(ARF)是急性髓系白血病(AML)患者入住重症监护病房(ICU)的主要原因,因此需要有关影响短期预后的预后因素的数据。
这是一项对入住ICU的免疫功能低下的ARF患者进行的多中心、国际前瞻性队列研究的事后分析。我们评估了AML和ARF患者的医院死亡率及相关危险因素;其次,我们旨在通过聚类分析在研究人群中确定特定亚组。
总体而言,1611例免疫功能低下的ARF患者中有201例患有AML并被纳入分析。医院死亡率为46.8%。与死亡率独立相关的变量包括:东部肿瘤协作组(ECOG)体能状态≥2(比值比[OR]=2.79,p=0.04)、咳嗽(OR=2.94,p=0.034)、使用血管升压药(OR=2.79,p=0.044)、白血病特异性肺部受累[即白细胞淤滞、原始细胞肺部浸润或急性溶解肺病(OR=4.76,p=0.011)]和肝脏序贯器官衰竭评估(SOFA)评分(OR=1.85,p=0.014)。局灶性肺泡胸部X线表现与生存相关(OR=0.13,p=0.001)。我们识别出3个聚类,根据每个聚类中最常见的临床、生物学和放射学特征将其命名:一个“白血病聚类”,包含患有孤立性、较轻ARF的高危AML患者;一个“肺部聚类”,由症状明显、高需氧、严重ARF且在免疫功能严重低下患者中具有弥漫性放射学表现的患者组成;一个临床“炎症聚类”,包括除ARF外还伴有多器官功能衰竭的患者。当纳入多变量分析时,聚类2和聚类3与医院死亡率独立相关。
在患有ARF的AML患者中,与较差预后相关的因素与患者背景(体能状态、白血病肺部受累)、症状、放射学表现、对血管升压药的需求以及肝脏SOFA评分有关。我们在AML患者中识别出三种特定的ARF综合征,它们具有预后意义,可指导临床医生优化管理策略。