Department of Public Health and Preventive Medicine, School of Medicine, Jinan University, Guangzhou, Guangdong, China.
Department of Medical Statistics & Epidemiology, International School of Public Health and One Health, Hainan Medical University, Haikou, Hainan, China.
Acta Obstet Gynecol Scand. 2023 Dec;102(12):1618-1633. doi: 10.1111/aogs.14648. Epub 2023 Sep 7.
The association between extreme birth spacing and adverse outcomes is controversial, and available evidence is fragmented into different classifications of birth spacing.
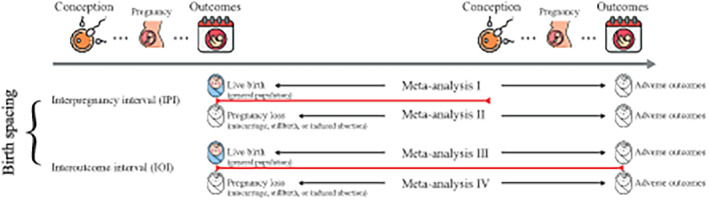
We conducted a systematic review of observational studies to evaluate the association between birth spacing (i.e., interpregnancy interval and interoutcome interval) and adverse outcomes (i.e., pregnancy complications, adverse birth outcomes). Pooled odds ratios (ORs) with 95% confidence intervals (CI) were calculated using a random-effects model, and the dose-response relationships were evaluated using generalized least squares trend estimation.
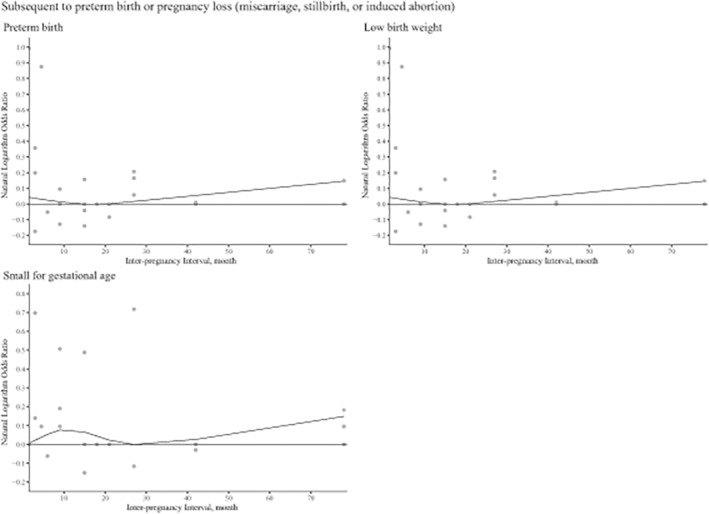
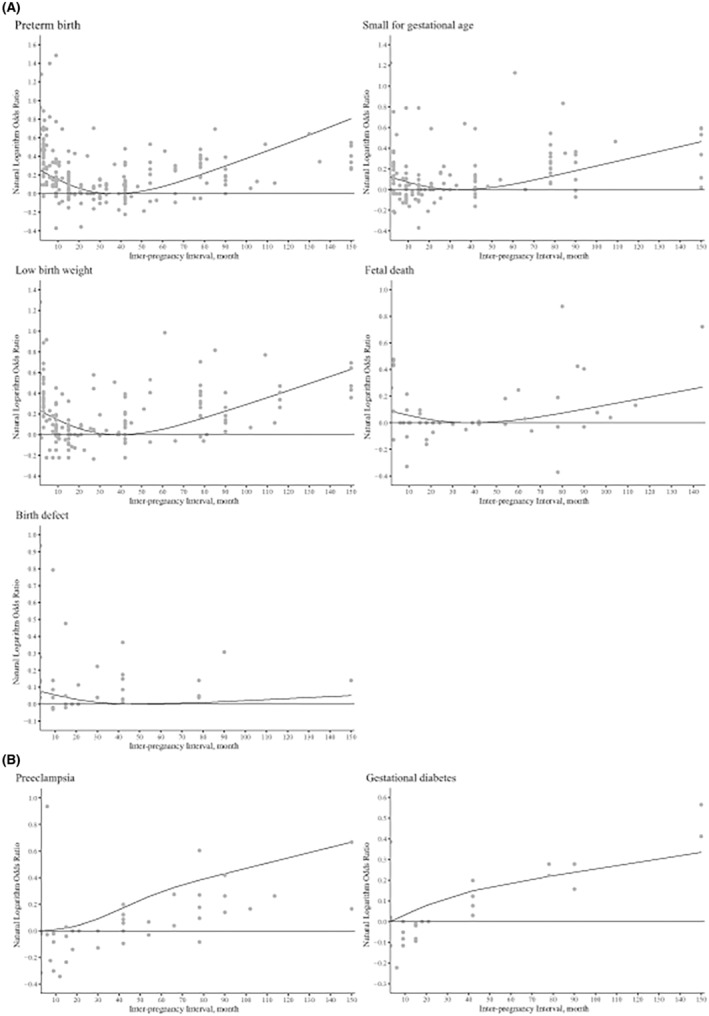
A total of 129 studies involving 46 874 843 pregnancies were included. In the general population, compared with an interpregnancy interval of 18-23 months, extreme intervals (<6 months and ≥ 60 months) were associated with an increased risk of adverse outcomes, including preterm birth, small for gestational age, low birthweight, fetal death, birth defects, early neonatal death, and premature rupture of fetal membranes (pooled OR range: 1.08-1.56; p < 0.05). The dose-response analyses further confirmed these J-shaped relationships (p < 0.001-0.009). Long interpregnancy interval was only associated with an increased risk of preeclampsia and gestational diabetes (p < 0.005 and p < 0.001, respectively). Similar associations were observed between interoutcome interval and risk of low birthweight and preterm birth (p < 0.001). Moreover, interoutcome interval of ≥60 months was associated with an increased risk of cesarean delivery (pooled OR 1.72, 95% CI 1.04-2.83). For pregnancies following preterm births, an interpregnancy interval of 9 months was not associated with an increased risk of preterm birth, according to dose-response analyses (p = 0.008). Based on limited evidence, we did not observe significant associations between interpregnancy interval or interoutcome interval after pregnancy losses and risk of small for gestational age, fetal death, miscarriage, or preeclampsia (pooled OR range: 0.76-1.21; p > 0.05).
Extreme birth spacing has extensive adverse effects on maternal and infant health. In the general population, interpregnancy interval of 18-23 months may be associated with potential benefits for both mothers and infants. For women with previous preterm birth, the optimal birth spacing may be 9 months.
极短生育间隔与不良结局之间的关联存在争议,现有证据碎片化为不同的生育间隔分类。
我们进行了一项系统综述,纳入了观察性研究,以评估生育间隔(即孕期间隔和产程间隔)与不良结局(即妊娠并发症、不良出生结局)之间的关联。采用随机效应模型计算合并优势比(OR)及其 95%置信区间(CI),并采用广义最小二乘趋势估计评估剂量-反应关系。
共纳入 129 项研究,涉及 46874843 例妊娠。在普通人群中,与孕期间隔 18-23 个月相比,极短间隔(<6 个月和≥60 个月)与早产、小于胎龄儿、低出生体重儿、胎儿死亡、出生缺陷、新生儿早期死亡和胎膜早破的风险增加相关(合并 OR 范围:1.08-1.56;p<0.05)。剂量-反应分析进一步证实了这些 J 型关系(p<0.001-0.009)。较长的孕期间隔仅与子痫前期和妊娠期糖尿病的风险增加相关(p<0.005 和 p<0.001)。产程间隔与低出生体重儿和早产的风险也存在类似的关联(p<0.001)。此外,产程间隔≥60 个月与剖宫产风险增加相关(合并 OR 1.72,95%CI 1.04-2.83)。对于早产分娩后的妊娠,根据剂量-反应分析,孕期间隔 9 个月与早产风险增加无关(p=0.008)。基于有限的证据,我们没有观察到孕期间隔或妊娠丢失后产程间隔与小于胎龄儿、胎儿死亡、流产或子痫前期风险之间存在显著关联(合并 OR 范围:0.76-1.21;p>0.05)。
极短生育间隔对母婴健康有广泛的不良影响。在普通人群中,孕期间隔 18-23 个月可能对母婴双方都有潜在的益处。对于有早产史的女性,最佳生育间隔可能为 9 个月。