Barbosa Maurício F, Canan Arzu, Xi Yin, Litt Harold, Diercks Deborah B, Abbara Suhny, Kay Fernando U
From the Department of Radiology, Cardiothoracic Division (M.F.B., A.C., S.A., F.U.K.), Department of Radiology (Y.X.), and Department of Emergency Medicine (D.B.D.), UT Southwestern Medical Center at Dallas, 5323 Harry Hines Blvd, Dallas, TX 75390; and Department of Radiology, University of Pennsylvania, Philadelphia, Pa (H.L.).
Radiol Cardiothorac Imaging. 2023 Aug 24;5(4):e230022. doi: 10.1148/ryct.230022. eCollection 2023 Aug.
To perform a living systematic review and meta-analysis of randomized controlled trials comparing the effectiveness of coronary CT angiography (CCTA) and standard of care (SOC) in the evaluation of acute chest pain (ACP).
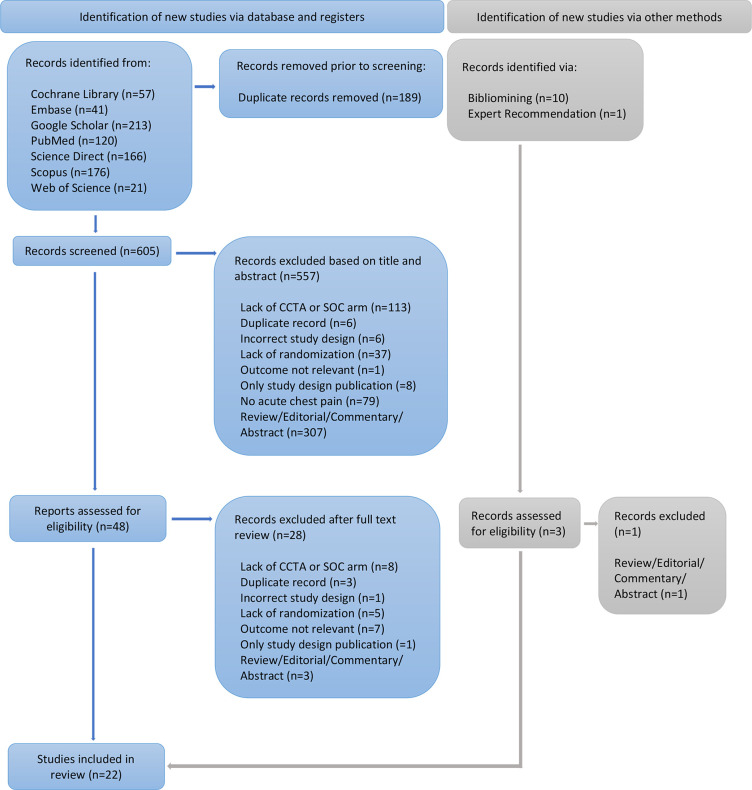
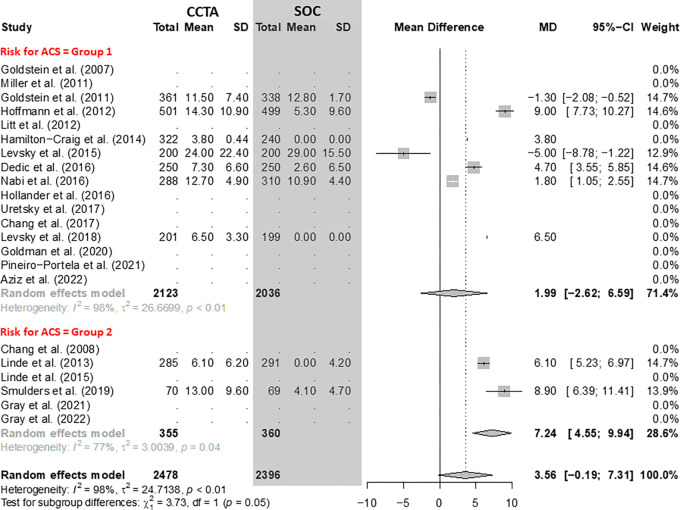
Multiple electronic databases were systematically searched, with the most recent search conducted on October 31, 2022. Studies were stratified into two groups according to the pretest probability for acute coronary syndrome (group 1 with predominantly low-to-intermediate risk vs group 2 with high risk). A meta-regression analysis was also conducted using participant risk, type of SOC used, and the use or nonuse of high-sensitivity troponins as independent variables.
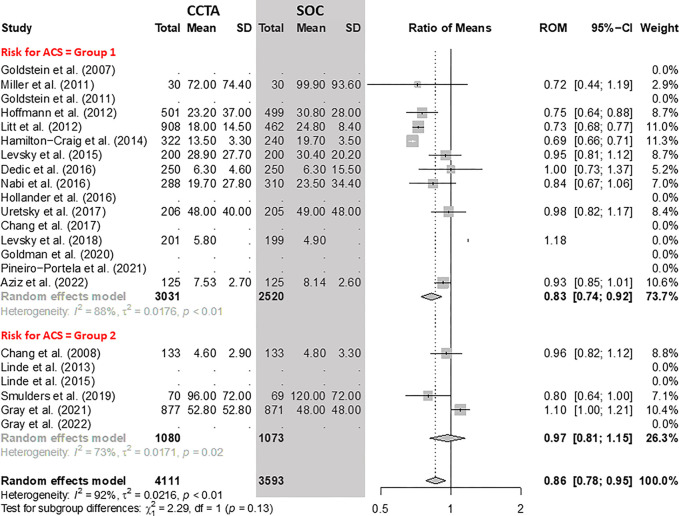
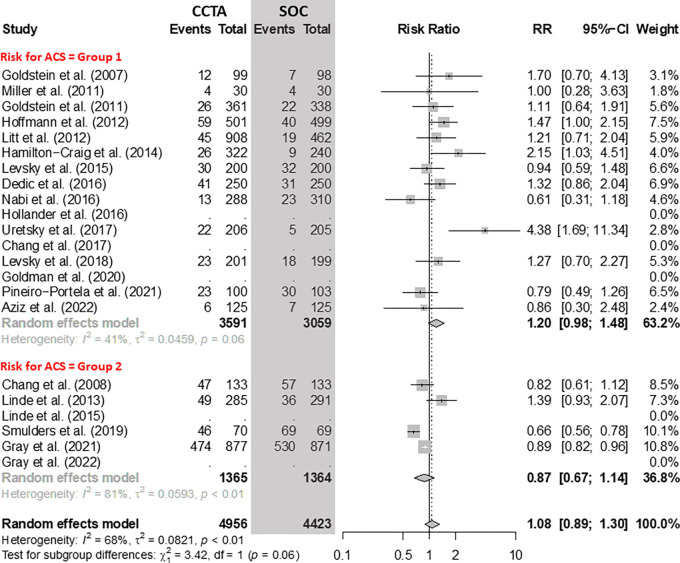
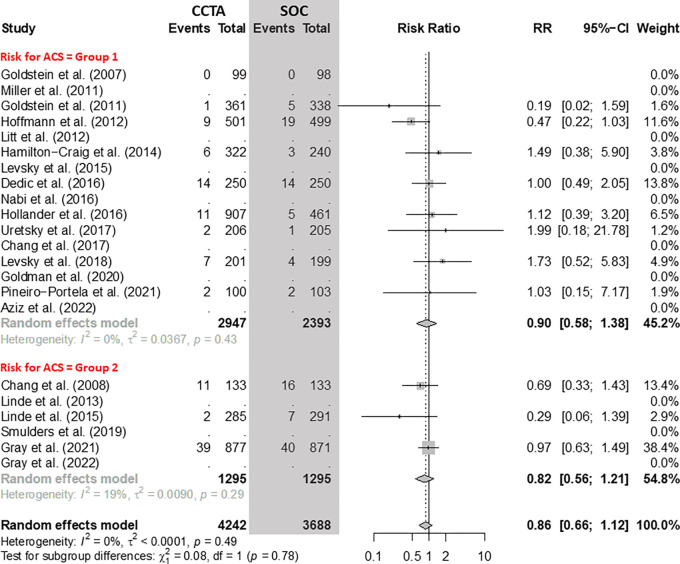
The final analysis included 22 randomized controlled trials (9379 total participants; 4956 assigned to CCTA arms and 4423 to SOC arms). There was a 14% reduction in the length of stay and a 17% reduction in immediate costs for the CCTA arm compared with the SOC arm. In group 1, the length of stay was 17% shorter and costs were 21% lower using CCTA. There was no evidence of differences in referrals to invasive coronary angiography, myocardial infarction, mortality, rate of hospitalization, further stress testing, or readmissions between CCTA and SOC arms. There were more revascularizations (relative risk, 1.45) and medication changes (relative risk, 1.33) in participants with low-to-intermediate acute coronary syndrome risk and increased radiation exposure in high-risk participants (mean difference, 7.24 mSv) in the CCTA arm compared with the SOC arm. The meta-regression analysis found significant differences between CCTA and SOC arms for rate of hospitalization, further stress testing, and medication changes depending on the type of SOC ( < .05).
The results support the use of CCTA as a safe, rapid, and less expensive in the short term strategy to exclude acute coronary syndrome in low- to intermediate-risk patients presenting with acute chest pain. Acute Coronary Syndrome, Chest Pain, Emergency Department, Coronary Computed Tomography, Usual Care Published under a CC BY 4.0 license.
对比较冠状动脉CT血管造影(CCTA)与标准治疗(SOC)在评估急性胸痛(ACP)方面有效性的随机对照试验进行实时系统评价和荟萃分析。
系统检索多个电子数据库,最近一次检索于2022年10月31日进行。根据急性冠状动脉综合征的预检概率将研究分为两组(第1组主要为低至中度风险,第2组为高风险)。还使用参与者风险、所使用的SOC类型以及是否使用高敏肌钙蛋白作为自变量进行了荟萃回归分析。
最终分析纳入了22项随机对照试验(共9379名参与者;4956名被分配至CCTA组,4423名被分配至SOC组)。与SOC组相比,CCTA组的住院时间缩短了14%,直接费用降低了17%。在第1组中,使用CCTA时住院时间缩短了17%,费用降低了21%。没有证据表明CCTA组和SOC组在侵入性冠状动脉造影转诊、心肌梗死、死亡率、住院率、进一步的压力测试或再入院方面存在差异。与SOC组相比,CCTA组中急性冠状动脉综合征风险为低至中度的参与者有更多的血运重建(相对风险,1.45)和药物变化(相对风险,1.33),高风险参与者的辐射暴露增加(平均差异,7.24 mSv)。荟萃回归分析发现,根据SOC类型,CCTA组和SOC组在住院率、进一步的压力测试和药物变化方面存在显著差异(P < .05)。
结果支持将CCTA作为一种安全、快速且短期成本较低的策略,用于排除急性胸痛的低至中度风险患者的急性冠状动脉综合征。急性冠状动脉综合征、胸痛、急诊科、冠状动脉计算机断层扫描、常规护理 依据知识共享署名4.0许可协议发布。