Nguyen Nam H, Dodd-Eaton Elissa B, Corredor Jessica L, Woodman-Ross Jacynda, Green Sierra, Hernandez Nathaniel D, Gutierrez Barrera Angelica M, Arun Banu K, Wang Wenyi
The University of Texas MD Anderson Cancer Center, Department of Bioinformatics and Computation Biology, Houston, TX.
Rice University, Department of Statistics, Houston, TX.
medRxiv. 2023 Sep 2:2023.08.31.23294849. doi: 10.1101/2023.08.31.23294849.
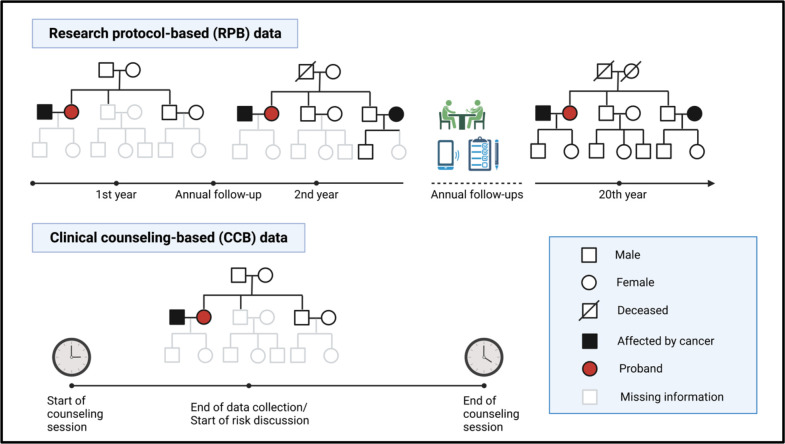
There exists a barrier between developing and disseminating risk prediction models in clinical settings. We hypothesize this barrier may be lifted by demonstrating the utility of these models using incomplete data that are collected in real clinical sessions, as compared to the commonly used research cohorts that are meticulously collected.
Genetic counselors (GCs) collect family history when patients (i.e., probands) come to MD Anderson Cancer Center for risk assessment of Li-Fraumeni syndrome, a genetic disorder characterized by deleterious germline mutations in the gene. Our clinical counseling-based (CCB) cohort consists of 3,297 individuals across 124 families (522 cases of single primary cancer and 125 cases of multiple primary cancers). We applied our software suite LFSPRO to make risk predictions and assessed performance in discrimination using area under the curve (AUC), and in calibration using observed/expected (O/E) ratio.
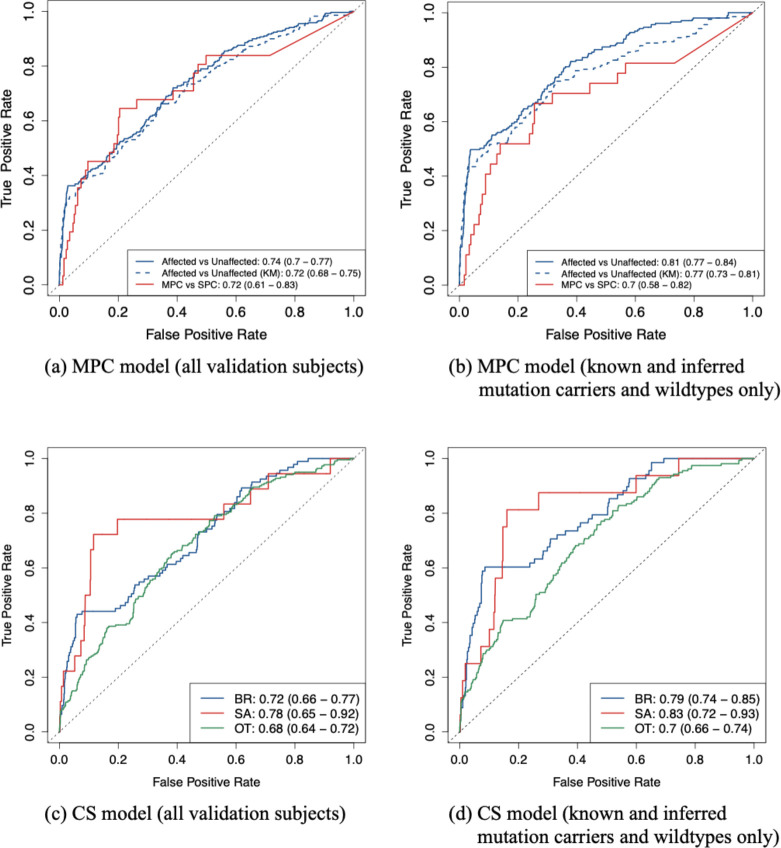
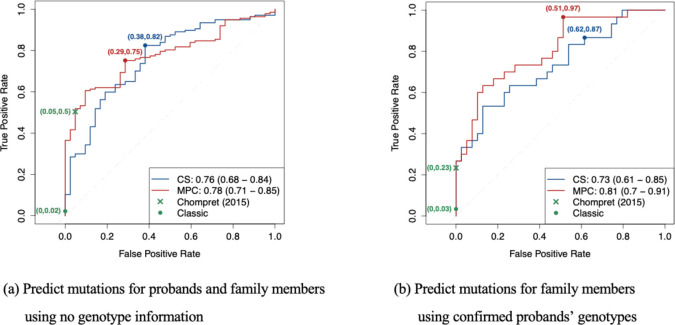
For prediction of deleterious mutations, we achieved an AUC of 0.81 (95% CI, 0.70 - 0.91) and an O/E ratio of 0.96 (95% CI, 0.70 - 1.21). Using the LFSPRO.MPC model to predict the onset of the second cancer, we obtained an AUC of 0.70 (95% CI, 0.58 - 0.82). Using the LFSPRO.CS model to predict the onset of different cancer types as the first primary, we achieved AUCs between 0.70 and 0.83 for sarcoma, breast cancer, or other cancers combined.
We describe a study that fills in the critical gap in knowledge for the utility of risk prediction models. Using a CCB cohort, our previously validated models have demonstrated good performance and outperformed the standard clinical criteria. Our study suggests better risk counseling may be achieved by GCs using these already-developed mathematical models.
在临床环境中,风险预测模型的开发与传播之间存在障碍。我们假设,与精心收集的常用研究队列相比,通过使用在实际临床过程中收集的不完整数据来证明这些模型的实用性,可能会消除这一障碍。
当患者(即先证者)前往MD安德森癌症中心进行李-弗劳梅尼综合征的风险评估时,遗传咨询师会收集家族病史,李-弗劳梅尼综合征是一种由该基因有害种系突变引起的遗传性疾病。我们基于临床咨询的(CCB)队列由124个家庭的3297名个体组成(522例单发原发性癌症和125例多发原发性癌症)。我们应用我们的软件套件LFSPRO进行风险预测,并使用曲线下面积(AUC)评估鉴别性能,使用观察值/期望值(O/E)比率评估校准性能。
对于有害突变的预测,我们获得的AUC为0.81(95%CI,0.70 - 0.91),O/E比率为0.96(95%CI,0.70 - 1.21)。使用LFSPRO.MPC模型预测第二种癌症的发病,我们获得的AUC为0.70(95%CI,0.58 - 0.82)。使用LFSPRO.CS模型预测不同癌症类型作为首发原发性癌症的发病,对于肉瘤、乳腺癌或其他癌症组合,我们获得的AUC在0.70至0.83之间。
我们描述了一项填补风险预测模型实用性知识关键空白的研究。使用CCB队列,我们先前验证的模型已证明具有良好的性能,并且优于标准临床标准。我们的研究表明,遗传咨询师使用这些已开发的数学模型可能会实现更好的风险咨询。