Department of Medicine, The University of Texas Southwestern Medical Center, Dallas, Texas, USA
Metroplex Clinical Research Center, Dallas, Texas, USA.
Ann Rheum Dis. 2023 Dec;82(12):1516-1526. doi: 10.1136/ard-2023-224482. Epub 2023 Sep 12.
To investigate the efficacy and safety of otilimab, an antigranulocyte-macrophage colony-stimulating factor antibody, in patients with active rheumatoid arthritis.
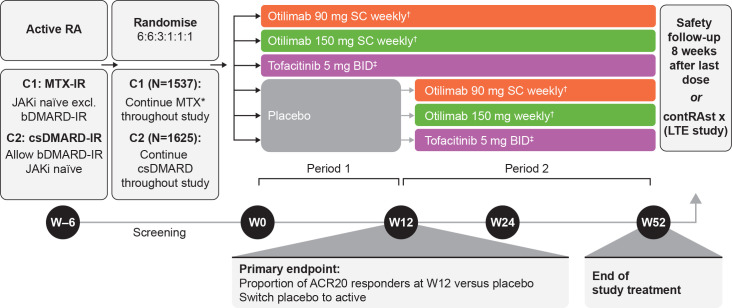
Two phase 3, double-blind randomised controlled trials including patients with inadequate responses to methotrexate (contRAst 1) or conventional synthetic/biologic disease-modifying antirheumatic drugs (cs/bDMARDs; contRAst 2). Patients received background csDMARDs. Through a testing hierarchy, subcutaneous otilimab (90/150 mg once weekly) was compared with placebo for week 12 endpoints (after which, patients receiving placebo switched to active interventions) or oral tofacitinib (5 mg two times per day) for week 24 endpoints.
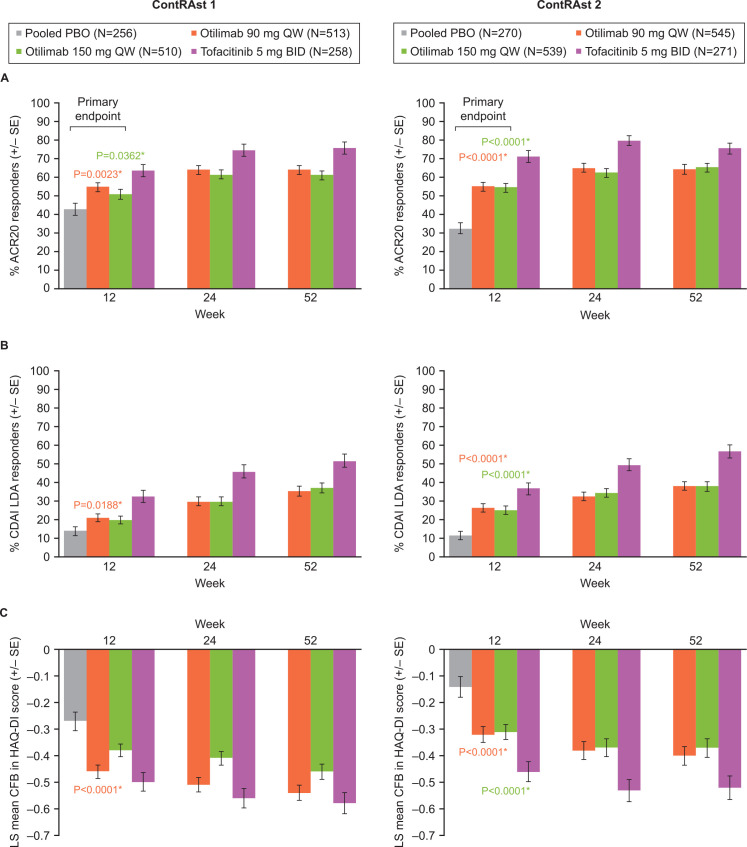
proportion of patients achieving an American College of Rheumatology response ≥20% (ACR20) at week 12.
The intention-to-treat populations comprised 1537 (contRAst 1) and 1625 (contRAst 2) patients.
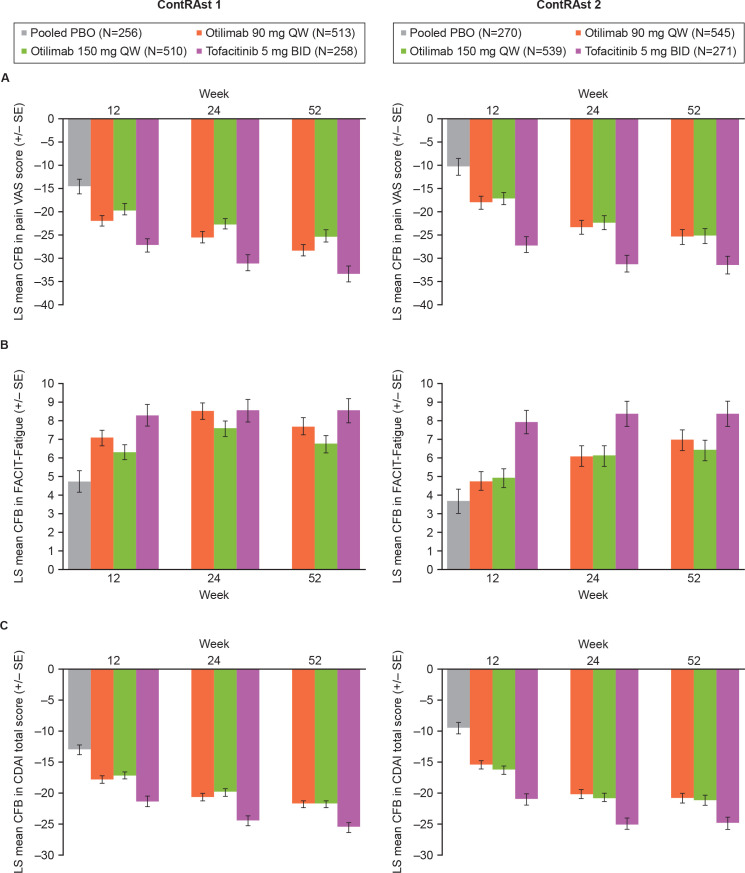
proportions of ACR20 responders were statistically significantly greater with otilimab 90 mg and 150 mg vs placebo in contRAst 1 (54.7% (p=0.0023) and 50.9% (p=0.0362) vs 41.7%) and contRAst 2 (54.9% (p<0.0001) and 54.5% (p<0.0001) vs 32.5%). Secondary endpoints: in both trials, compared with placebo, otilimab increased the proportion of Clinical Disease Activity Index (CDAI) low disease activity (LDA) responders (not significant for otilimab 150 mg in contRAst 1), and reduced Health Assessment Questionnaire-Disability Index (HAQ-DI) scores. Benefits with tofacitinib were consistently greater than with otilimab across multiple endpoints. Safety outcomes were similar across treatment groups.
Although otilimab demonstrated superiority to placebo in ACR20, CDAI LDA and HAQ-DI, improved symptoms, and had an acceptable safety profile, it was inferior to tofacitinib.
NCT03980483, NCT03970837.
评估抗粒细胞-巨噬细胞集落刺激因子抗体奥替利珠单抗在活动性类风湿关节炎患者中的疗效和安全性。
这两项 3 期、双盲随机对照试验纳入了对甲氨蝶呤应答不足的患者(contRAst 1)或常规合成/生物改善病情抗风湿药物(cs/bDMARDs;contRAst 2)应答不足的患者。患者接受背景 csDMARDs 治疗。通过检测分层,每周皮下注射奥替利珠单抗(90/150 mg,每周一次)与安慰剂比较,以达到第 12 周终点(此后,接受安慰剂的患者转为活性干预),或每周 24 周终点时口服托法替布(5 mg,每日两次)。
第 12 周时达到美国风湿病学会 20%应答(ACR20)的患者比例。
意向治疗人群包括 1537 名(contRAst 1)和 1625 名(contRAst 2)患者。
奥替利珠单抗 90 mg 和 150 mg 与安慰剂相比,在 contRAst 1 中达到 ACR20 应答的患者比例具有统计学显著意义(54.7%(p=0.0023)和 50.9%(p=0.0362)vs 41.7%)和 contRAst 2(54.9%(p<0.0001)和 54.5%(p<0.0001)vs 32.5%)。次要终点:与安慰剂相比,在两项试验中,奥替利珠单抗均增加了临床疾病活动指数(CDAI)低疾病活动(LDA)应答者的比例(奥替利珠单抗 150 mg 在 contRAst 1 中不显著),并降低了健康评估问卷残疾指数(HAQ-DI)评分。与奥替利珠单抗相比,托法替布在多个终点的疗效均更为显著。各组治疗的安全性结局相似。
尽管奥替利珠单抗在 ACR20、CDAI LDA 和 HAQ-DI 方面优于安慰剂,改善了症状,且具有可接受的安全性,但它不如托法替布。
NCT03980483、NCT03970837。