Wang Rui, Liu Ya, Liang Yan, Zhou Li, Chen Mao-Jia, Liu Xu-Bao, Tan Chun-Lu, Chen Yong-Hua
Division of Pancreatic Surgery, Department of General Surgery, West China Hospital, Sichuan University, Chengdu 610041, Sichuan Province, China.
Department of General Surgery, Chengdu Second People's Hospital, Chengdu 610041, Sichuan Province, China.
World J Gastrointest Surg. 2023 Aug 27;15(8):1703-1711. doi: 10.4240/wjgs.v15.i8.1703.
Islet amyloid deposition and reduced β-cell mass are pathological hallmarks in type 2 diabetes mellitus subjects. To date, the pathological features of the islets in diabetes secondary to pancreatic ductal adenocarcinoma (PDAC) have not been specifically addressed.
To provide further insight into the relationship between islet amyloid deposition of the residual pancreas in PDAC patients and to explore whether regional differences (proximal distal residual pancreas) are associated with islet amyloid deposition.
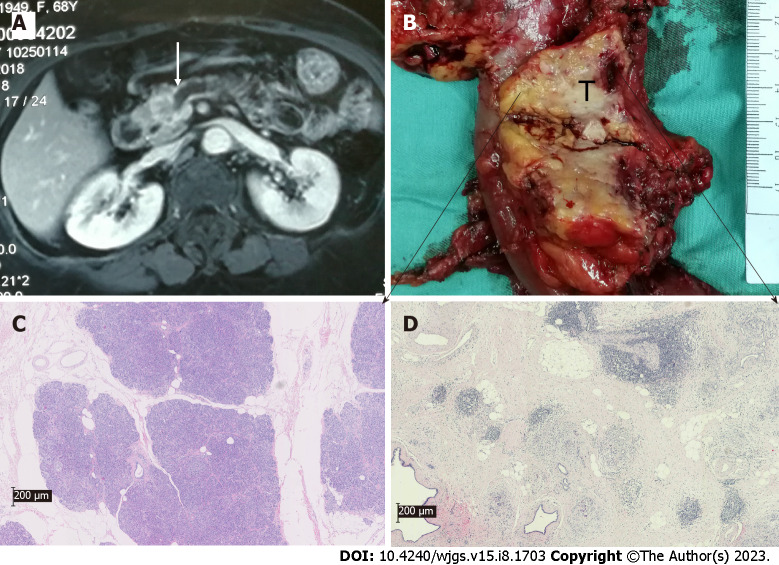
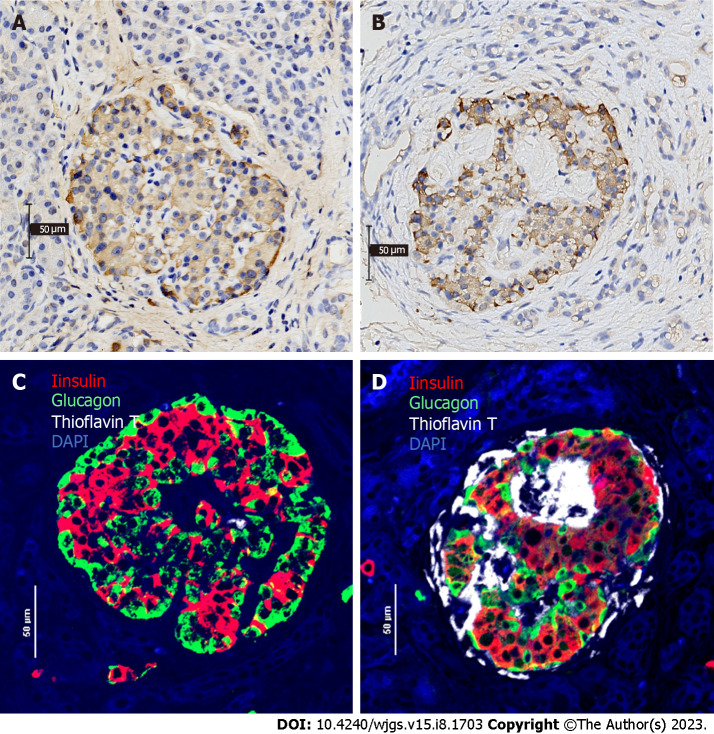
We retrospectively collected clinical information and pancreatic tissue removed from tumors of 45 PDAC patients, including 14 patients with normal glucose tolerance (NGT), 16 patients with prediabetes and 15 new-onset diabetes (NOD) patients diagnosed before surgery by an oral glucose tolerance test at West China Hospital from July 2017 to June 2020. Pancreatic volume was calculated by multiplying the estimated area of pancreatic tissue on each image slice by the interval between slices based on abdominal computer tomography scans. Several sections of paraffin-embedded pancreas specimens from both the proximal and/or distal regions remote from the tumor were stained as follows: (1) Hematoxylin and eosin for general histological appearance; (2) hematoxylin and insulin for the determination of fractional β-cell area (immunohistochemistry); and (3) quadruple insulin, glucagon, thioflavin T and DAPI staining for the determination of β-cell area, α-cell area and amyloid deposits.
Screening for pancreatic histologic features revealed that duct obstruction with islet amyloid deposition, fibrosis and marked acinar atrophy were robust in the distal pancreatic regions but much less robust in the proximal regions, especially in the prediabetes and NOD groups. Consistent with this finding, the remnant pancreatic volume was markedly decreased in the NOD group by nearly one-half compared with that in the NGT group (37.35 ± 12.16 cm 69.79 ± 18.17 cm, < 0.001). As expected, islets that stained positive for amyloid (islet amyloid density) were found in the majority of PDAC cases. The proportion of amyloid/islet area (severity of amyloid deposition) was significantly higher in both prediabetes and NOD patients than in NGT patients ( = 0.002; < 0.0001, respectively). We further examined the regional differences in islet amyloid deposits. Islet amyloid deposit density was robustly increased by approximately 8-fold in the distal regions compared with that in the proximal regions in the prediabetes and NOD groups (3.98% ± 3.39% 0.50% ± 0.72%, = 0.01; 12.03% 1.51%, = 0.001, respectively).
In conclusion, these findings suggest that robust alterations of the distal pancreas due to tumors can disturb islet function and structure with islet amyloid formation, which may be associated with the pathogenesis of NOD secondary to PDAC.
胰岛淀粉样变沉积和β细胞数量减少是2型糖尿病患者的病理特征。迄今为止,胰腺导管腺癌(PDAC)继发糖尿病患者胰岛的病理特征尚未得到专门研究。
进一步了解PDAC患者残余胰腺的胰岛淀粉样变沉积之间的关系,并探讨区域差异(近端与远端残余胰腺)是否与胰岛淀粉样变沉积有关。
我们回顾性收集了2017年7月至2020年6月在华西医院接受手术的45例PDAC患者的临床信息和肿瘤切除的胰腺组织,其中包括14例糖耐量正常(NGT)患者、16例糖尿病前期患者和15例新诊断糖尿病(NOD)患者,术前通过口服葡萄糖耐量试验进行诊断。根据腹部计算机断层扫描,将每个图像切片上胰腺组织的估计面积乘以切片间隔来计算胰腺体积。从远离肿瘤的近端和/或远端区域获取的几个石蜡包埋胰腺标本切片进行如下染色:(1)苏木精和伊红染色用于观察一般组织学外观;(2)苏木精和胰岛素染色用于测定β细胞面积分数(免疫组织化学);(3)胰岛素、胰高血糖素、硫黄素T和DAPI四重染色用于测定β细胞面积、α细胞面积和淀粉样沉积物。
胰腺组织学特征筛查显示,胰岛淀粉样变沉积、纤维化和明显的腺泡萎缩导致的导管阻塞在胰腺远端区域较为明显,但在近端区域则不那么明显,尤其是在糖尿病前期和NOD组。与这一发现一致,NOD组的残余胰腺体积与NGT组相比明显减少了近一半(37.35±12.16 cm³对69.79±18.17 cm³,P<0.001)。正如预期的那样,大多数PDAC病例中发现胰岛淀粉样变染色呈阳性(胰岛淀粉样密度)。糖尿病前期和NOD患者的淀粉样物质/胰岛面积比例(淀粉样变沉积严重程度)均显著高于NGT患者(分别为P = 0.002;P<0.0001)。我们进一步检查了胰岛淀粉样变沉积物的区域差异。糖尿病前期和NOD组中,远端区域的胰岛淀粉样变沉积密度比近端区域显著增加了约8倍(分别为3.98%±3.39%对0.50%±0.72%,P = 0.01;12.03%对1.51%,P = 0.001)。
总之,这些发现表明,肿瘤导致的远端胰腺显著改变可通过胰岛淀粉样变形成干扰胰岛功能和结构,这可能与PDAC继发NOD的发病机制有关。