Karl Landsteiner University of Health Sciences, Dr. Karl-Dorrek-Straße 30, Krems, 3500, Austria.
Division of Internal Medicine, Gastroenterology & Hepatology, University Hospital of St. Pölten, Dunant-Platz 1, St. Pölten, A - 3100, Austria.
BMC Gastroenterol. 2023 Sep 15;23(1):314. doi: 10.1186/s12876-023-02942-w.
Validated, accepted grading tools for preprocedural complexity assessment in ERCP are lacking. We therefore created a grading system for ERCP based on the classification used by the American Society for Gastrointestinal Endoscopy (ASGE).
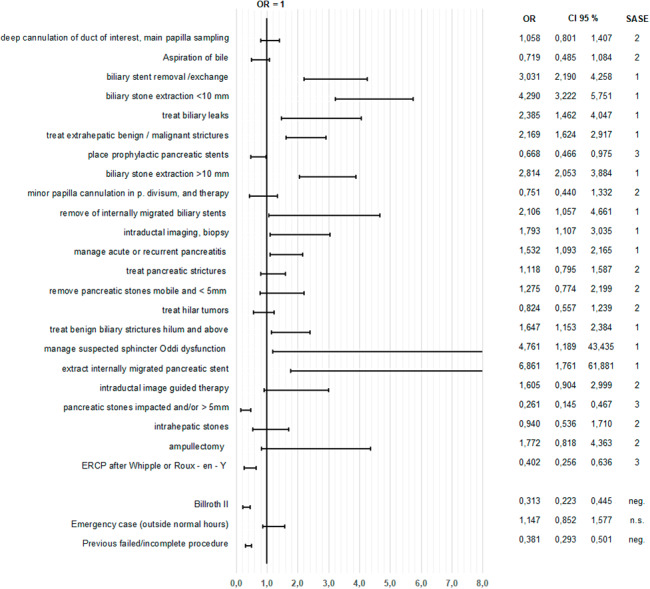
Data on ERCP adverse events (AE) and success were collected in a multicenter, prospective uncontrolled study. Multiple logistic regressions were applied to success and AEs in accordance with the ASGE classification. Each procedure suggested by ASGE was tested against different outcomes. Results were used to create a score and were evaluated in a control cohort.
16,327 ERCPs were documented in 27 centers. Analysis of ASGE categorization (10,904 cases) showed that this model fails to adequately predict parameters of complexity; only for cardiopulmonary AEs and perforation was no significant variance evident. Depending on the specific clinical circumstances, probability of success of the intervention sometimes varied significantly in risk, implying a twofold score, one part for probability of success and one for risk. A split score with three levels each was designed and tested in a validation cohort (5,423 procedures). Achieving therapeutic targets / post-ERCP pancreatitis could be correctly predicted in 87.0%/95.3%.
Grading ERCP success and AEs have to be considered independently. Onefold grading systems appear incomplete and unable to provide an adequate classification of severity. SASE (Success and Adverse Event Score in Endoscopic Retrograde Cholangiopancreatography) was created to incorporate these findings. Showing high predictive value, this score could be a potent tool for planning ERCP and training in endoscopy.
缺乏经过验证、可接受的 ERCP 术前复杂程度评估分级工具。因此,我们根据美国胃肠内镜学会(ASGE)的分类创建了一种基于 ERCP 的分级系统。
在一项多中心前瞻性非对照研究中收集了 ERCP 不良事件(AE)和成功率的数据。根据 ASGE 分类,对成功率和 AE 应用多变量逻辑回归。根据 ASGE 提出的每一项操作,测试不同的结果。使用结果创建评分,并在对照队列中进行评估。
在 27 个中心记录了 16327 例 ERCP。对 ASGE 分类(10904 例)的分析表明,该模型不能充分预测复杂程度参数;只有心肺 AE 和穿孔没有明显的差异。根据具体的临床情况,干预成功率的风险有时会有很大的差异,这意味着需要两倍的评分,一部分是成功率,一部分是风险。设计并在验证队列(5423 例)中测试了一个三分制的分割评分。治疗目标/内镜逆行胰胆管造影后胰腺炎的达成可以正确预测 87.0%/95.3%。
ERCP 成功率和 AE 的分级必须独立考虑。单一评分系统似乎不完整,无法提供充分的严重程度分类。SASE(内镜逆行胰胆管造影中的成功率和不良事件评分)的创建是为了纳入这些发现。该评分具有较高的预测价值,可能是规划 ERCP 和内镜培训的有力工具。