Sun Lei, Zhao Qi, Wang Yanning, Wang Yongsheng, Zheng Ming, Ding Xuansheng, Miao Liyun
School of Basic Medicine and Clinical Pharmacy, China Pharmaceutical University Nanjing Drum Tower Hospital, Nanjing, People's Republic of China.
Department of Respiratory and Critical Care Medicine, Nanjing Drum Tower Hospital, The Affiliated Hospital of Nanjing University Medical School, Nanjing, People's Republic of China.
Int J Gen Med. 2023 Sep 12;16:4165-4179. doi: 10.2147/IJGM.S424777. eCollection 2023.
Anlotinib is widely used in the clinical treatment of non-small cell lung cancer (NSCLC), alone or in combination with other anticancer drugs. The aim of this study was to investigate the real-world efficacy and safety of anlotinib-containing regimens.
Confirmed advanced NSCLC patients who had received anlotinib alone or in combination were enrolled. An overall analysis of the efficacy and safety of anlotinib was performed in all patients, and then subgroup analysis was used to further compare the efficacy between anlotinib monotherapy and combination therapy. The primary endpoint was progression-free survival (PFS), and the secondary endpoints were ADR, ORR, and DCR.
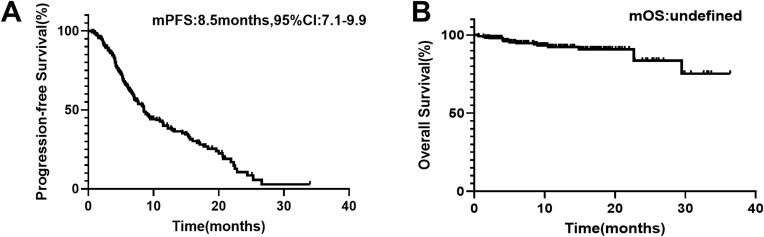
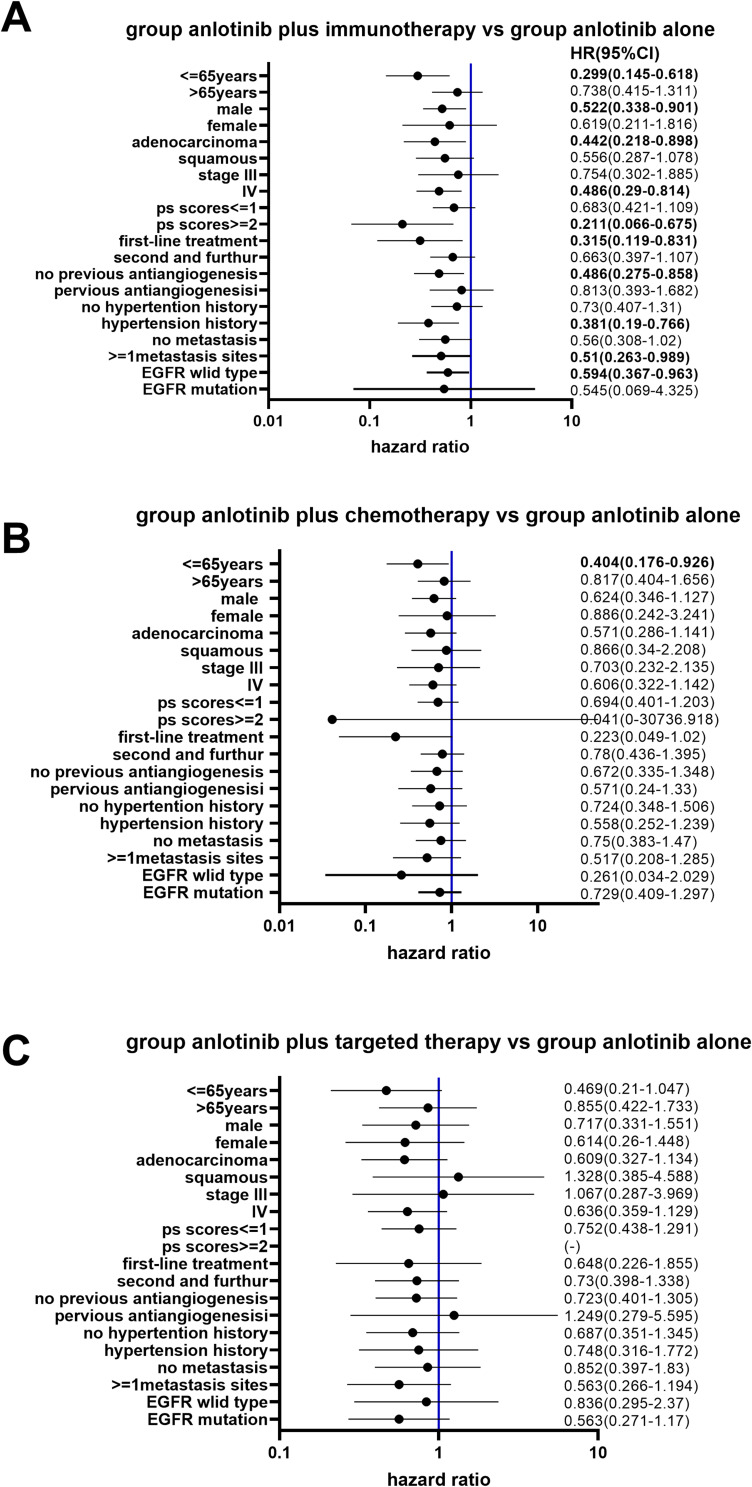
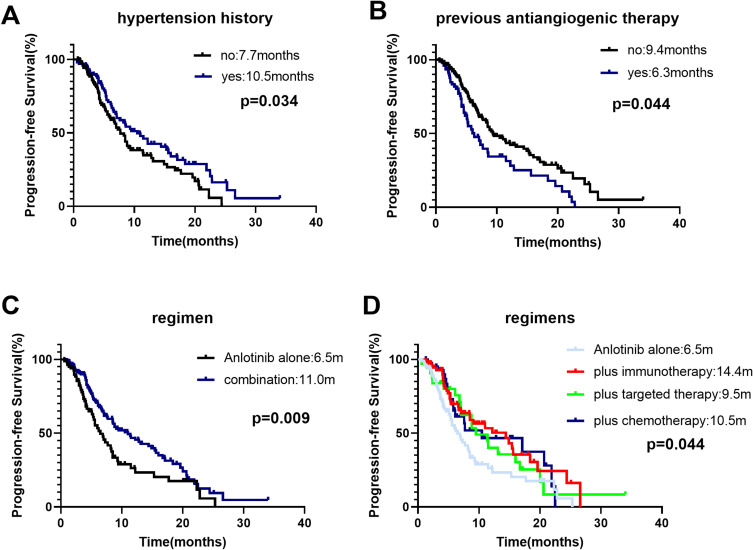
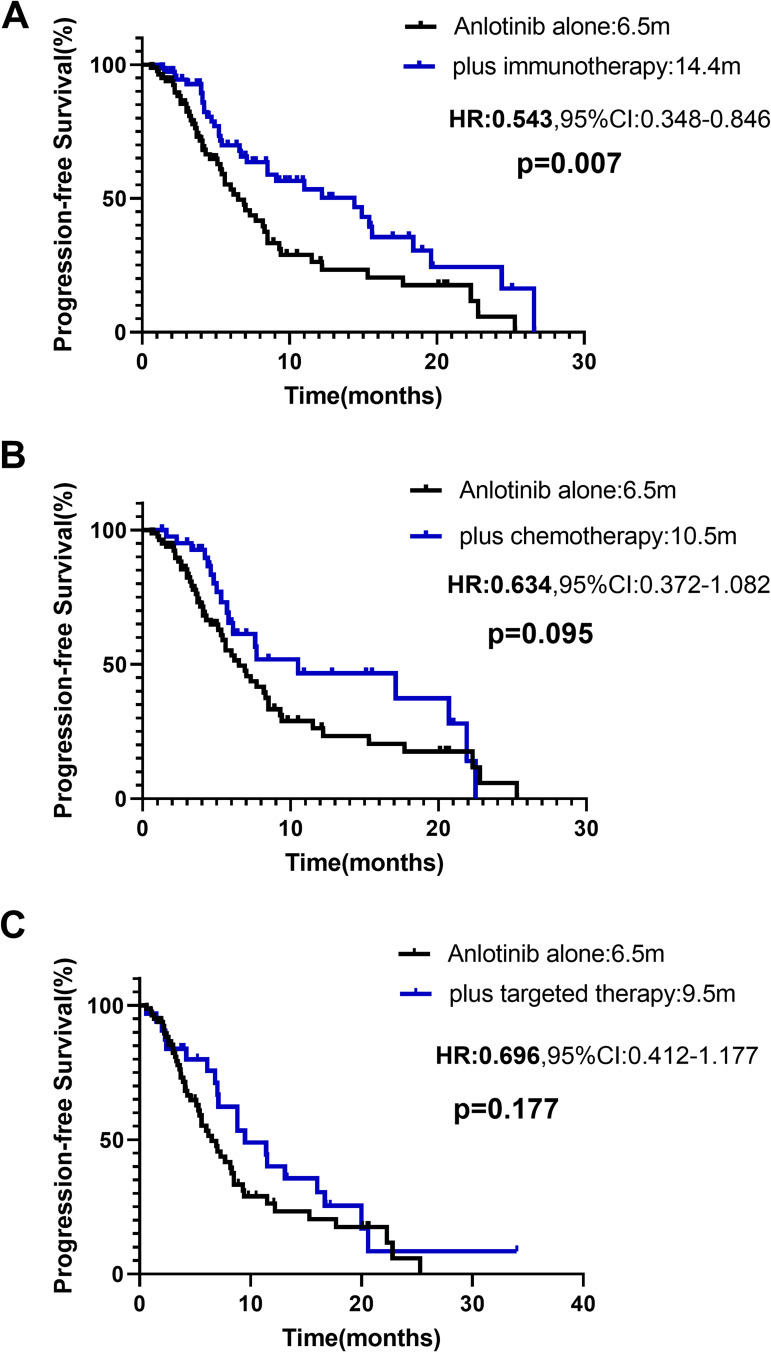
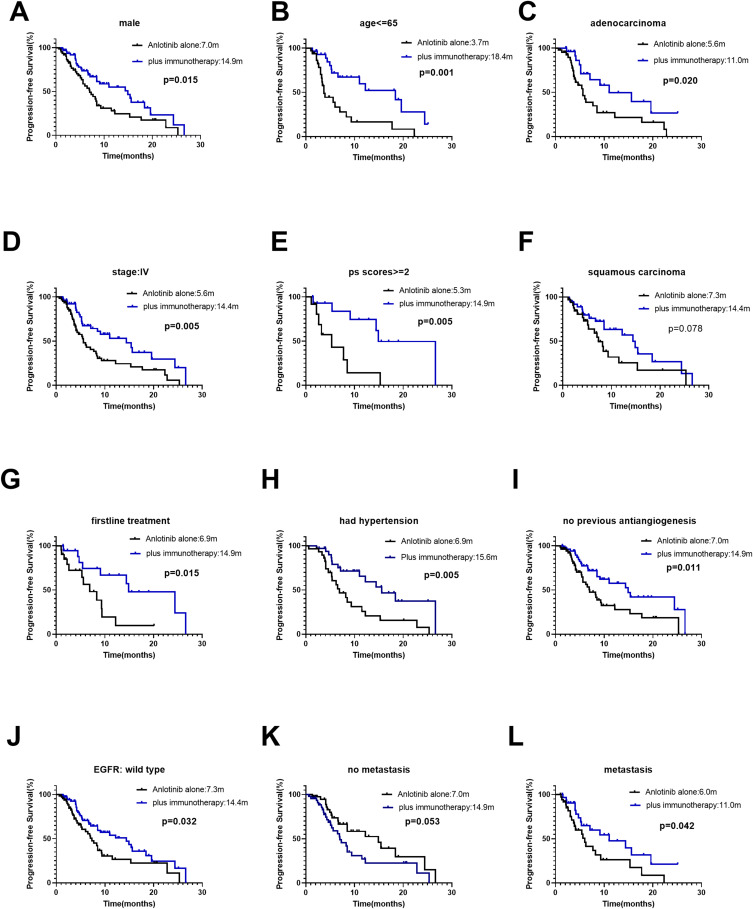
A total of 240 patients were included. The overall median PFS was 8.5 months (95% confidence interval [CI]: 7.1-9.9 months). Anlotinib treatment regimens (monotherapy or combination therapy) and whether they received previous antiangiogenesis were associated with PFS. Anlotinib plus immunotherapy achieved longer PFS than anlotinib monotherapy (median PFS: 10.5 vs 6.5 months, p=0.007). Stratification analysis showed the PFS of anlotinib plus immunotherapy was significantly longer in male, adenocarcinoma, <=65 years old, patients stage IV, EGFR wild type, with extrathoracic metastasis, performance status scores ≥2, the first-line treatment, patients with a history of hypertension and no previous antiangiogenesis than anlotinib monotherapy. The median PFS of anlotinib plus chemotherapy, targeted therapy was slightly longer than anlotinib alone (respectively, 10.5 vs 6.5 months, p=0.095; 9.5 vs 6.5 months, p=0.177). Adverse reactions were mostly mild and acceptable, with hypertension being the most common.
Anlotinib is effective and tolerable in advanced NSCLC patients. Immunotherapy combination with anlotinib significantly improved PFS. The efficacy of anlotinib may be impaired by previous antiangiogenic therapy, which can be investigated in further studies.
安罗替尼广泛应用于非小细胞肺癌(NSCLC)的临床治疗,可单独使用或与其他抗癌药物联合使用。本研究旨在探讨含安罗替尼方案的真实世界疗效和安全性。
纳入确诊的晚期NSCLC患者,这些患者单独或联合使用过安罗替尼。对所有患者进行安罗替尼疗效和安全性的总体分析,然后进行亚组分析以进一步比较安罗替尼单药治疗与联合治疗之间的疗效。主要终点为无进展生存期(PFS),次要终点为不良反应(ADR)、客观缓解率(ORR)和疾病控制率(DCR)。
共纳入240例患者。总体中位PFS为8.5个月(95%置信区间[CI]:7.1 - 9.9个月)。安罗替尼治疗方案(单药治疗或联合治疗)以及是否接受过先前的抗血管生成治疗与PFS相关。安罗替尼联合免疫治疗的PFS长于安罗替尼单药治疗(中位PFS:10.5 vs 6.5个月,p = 0.007)。分层分析显示,安罗替尼联合免疫治疗在男性、腺癌、≤65岁、IV期患者、EGFR野生型、有胸外转移、体能状态评分≥2、一线治疗、有高血压病史且未接受过先前抗血管生成治疗的患者中,PFS显著长于安罗替尼单药治疗。安罗替尼联合化疗、靶向治疗的中位PFS略长于安罗替尼单药治疗(分别为10.5 vs 6.5个月,p = 0.095;9.5 vs 6.5个月,p = 0.177)。不良反应大多轻微且可接受,高血压最为常见。
安罗替尼在晚期NSCLC患者中有效且耐受性良好。免疫治疗与安罗替尼联合可显著改善PFS。先前的抗血管生成治疗可能会损害安罗替尼的疗效,这可在进一步研究中进行探讨。