Centre for Infectious Disease Control, National Institute for Public Health and the Environment, Bilthoven, The Netherlands
Centre for Infectious Disease Control, National Institute for Public Health and the Environment, Bilthoven, The Netherlands.
BMJ Open. 2023 Sep 18;13(9):e072862. doi: 10.1136/bmjopen-2023-072862.
Targeted testing policy for HIV/syphilis at Dutch sexual health centres (SHCs) was evaluated for its efficiency in younger heterosexuals but not for heterosexuals ≥25 years. Currently, all older heterosexuals are tested for HIV/syphilis at SHCs. To explore possibilities for increased efficiency of testing in heterosexuals aged >25 years, this study aimed to identify determinants of HIV and syphilis diagnoses that could be used in targeted testing strategies.
An observational study using surveillance data from all Dutch SHC.
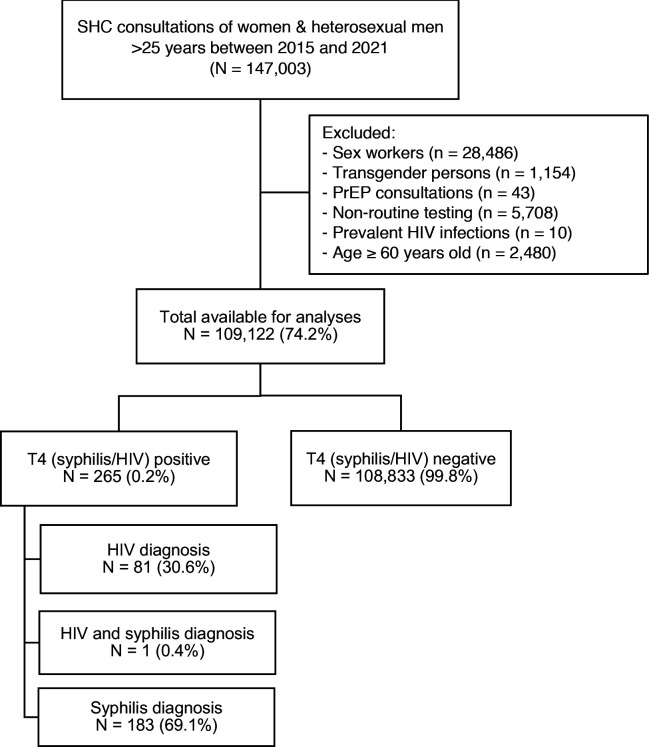
Women and heterosexual men aged >25 years visiting SHC between 2015 and 2021.
The primary outcome was HIV/syphilis diagnosis, determinants of a diagnosis were analysed. Based on these determinants and their applicability in SHC practice, different targeted testing scenarios were evaluated. For each scenario, the percentage of consultations involving HIV and syphilis testing and the total amount of missed HIV and syphilis diagnoses were calculated.
109 122 consultations were included among 75 718 individuals. The strongest determinants of HIV/syphilis diagnosis were HIV/syphilis-specific symptoms (adjusted OR (aOR) 34.9 (24.1-50.2)) and receiving partner notification (aOR 18.3 (13.2-25.2)), followed by low/middle education level (aOR 2.8 (2.0-4.0)), male sex (aOR 2.2 (1.6-3.0)) and age ≥30 years (aOR 1.8 (1.3-2.5)). When applying feasible determinants to targeted testing scenarios, HIV/syphilis testing would have been conducted in 54.5% of all consultations, missing 2 HIV and 3 syphilis diagnoses annually (13.4% and 11.4% of all diagnoses, respectively). In the scenario with the lowest number of missed HIV/syphilis diagnoses (0.3 HIV and 2 syphilis diagnoses annually), HIV/syphilis testing would have been conducted in 74.2% of all consultations.
In any targeted testing scenario studied, HIV and/or syphilis diagnoses would have been missed. This raises the question whether it is acceptable to put any of these scenarios into practice. This study contributes to a discussion about the impact of targeted testing policy.
评估荷兰性健康中心(SHC)针对 HIV/梅毒的靶向检测政策在年轻异性恋者中的效率,但未评估其在≥25 岁的异性恋者中的效率。目前,所有≥25 岁的年长异性恋者都在 SHC 接受 HIV/梅毒检测。为了探索提高≥25 岁异性恋者检测效率的可能性,本研究旨在确定可用于靶向检测策略的 HIV 和梅毒诊断的决定因素。
一项使用所有荷兰 SHC 的监测数据进行的观察性研究。
2015 年至 2021 年间在 SHC 就诊的年龄>25 岁的女性和异性恋男性。
主要结局是 HIV/梅毒诊断,分析了诊断的决定因素。基于这些决定因素及其在 SHC 实践中的适用性,评估了不同的靶向检测方案。对于每种方案,计算了涉及 HIV 和梅毒检测的咨询百分比和错过的 HIV 和梅毒诊断总数。
在纳入的 75718 名个体中,共纳入了 109122 次就诊。HIV/梅毒诊断的最强决定因素是 HIV/梅毒特异性症状(调整后的比值比[aOR]34.9[24.1-50.2])和接受伴侣通知(aOR 18.3[13.2-25.2]),其次是低/中等教育水平(aOR 2.8[2.0-4.0])、男性(aOR 2.2[1.6-3.0])和年龄≥30 岁(aOR 1.8[1.3-2.5])。当将可行的决定因素应用于靶向检测方案时,将对所有咨询的 54.5%进行 HIV/梅毒检测,每年将错过 2 例 HIV 和 3 例梅毒诊断(分别占所有诊断的 13.4%和 11.4%)。在错过 HIV/梅毒诊断数量最少的方案(每年 0.3 例 HIV 和 2 例梅毒诊断)中,将对所有咨询的 74.2%进行 HIV/梅毒检测。
在所研究的任何靶向检测方案中,都可能会错过 HIV 和/或梅毒的诊断。这引发了一个问题,即将任何这些方案付诸实践是否可以接受。本研究有助于讨论靶向检测政策的影响。