Department of Public Health, Erasmus MC, University Medical Center Rotterdam, Rotterdam, The Netherlands.
Department of Public Health, Municipal Public Health Service Rotterdam-Rijnmond, P.O. Box 70032, Rotterdam, 3000 LP, The Netherlands.
BMC Public Health. 2023 Dec 21;23(1):2553. doi: 10.1186/s12889-023-17483-w.
Access to HIV testing is crucial for detection, linkage to treatment, and prevention. In less urbanised areas, reliance on general practitioners (GPs) for HIV testing is probable, as sexual health centres (SHC) are mostly located within urbanised areas. Limited insight into individuals undergoing HIV testing stems from sparse standard registration of demographics at GPs. This cross-sectional study aims (1) to assess and compare HIV testing at the GP and SHC, and (2) to assess population- and provider-specific HIV incidence.
Individual HIV testing data of GPs and SHC were linked to population register data (aged ≥ 15 years, Rotterdam area, 2015-2019). We reported the proportion HIV tested, and compared GP and SHC testing rates with negative binomial generalised additive models. Data on new HIV diagnoses (2015-2019) from the Dutch HIV Monitoring Foundation relative to the population were used to assess HIV incidence.
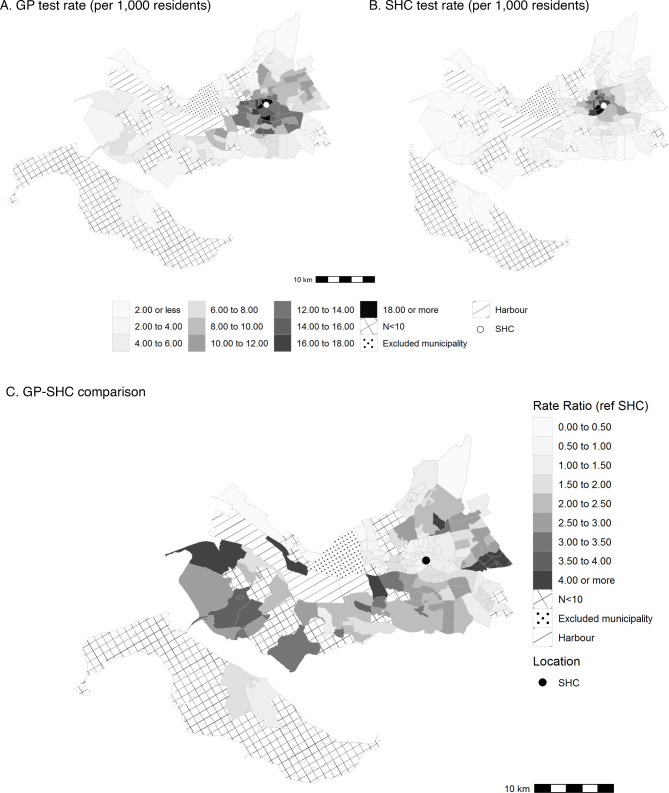
The overall proportion HIV tested was 1.14% for all residents, ranging from 0.41% for ≥ 40-year-olds to 4.70% for Antilleans. The GP testing rate was generally higher than the SHC testing rate with an overall rate ratio (RR) of 1.61 (95% CI: 1.56-1.65), but not for 15-24-year-olds (RR: 0.81, 95% CI: 0.74-0.88). Large differences in HIV testing rate (1.36 to 39.47 per 1,000 residents) and GP-SHC ratio (RR: 0.23 to 7.24) by geographical area were observed. The GPs' contribution in HIV testing was greater for GP in areas further away from the SHC. In general, population groups that are relatively often tested are also the groups with most diagnoses and highest incidence (e.g., men who have sex with men, non-western). The overall incidence was 10.55 per 100,000 residents, varying from 3.09 for heterosexual men/women to 24.04 for 25-29-year-olds.
GPs have a pivotal role in HIV testing in less urbanised areas further away from the SHC, and among some population groups. A relatively high incidence often follows relatively high testing rates. Opportunities to improve HIV testing have been found for migrants, lower-educated individuals, in areas less urbanised areas and further away from GP/SHC. Strategies include additional targeted testing, via for example SHC branch locations and outreach activities.
获得 HIV 检测对于发现、与治疗机构建立联系和预防至关重要。在欠发达的地区,可能依赖全科医生(GP)进行 HIV 检测,因为性健康中心(SHC)大多位于城市地区。由于在 GP 处对人口统计学数据的标准登记有限,因此对接受 HIV 检测的个体的了解甚少。本横断面研究旨在:(1)评估和比较 GP 和 SHC 的 HIV 检测情况,(2)评估人群和提供者特异性 HIV 发病率。
将 GP 和 SHC 的个体 HIV 检测数据与人口登记数据(年龄≥15 岁,鹿特丹地区,2015-2019 年)进行关联。我们报告了接受 HIV 检测的比例,并使用负二项式广义加性模型比较了 GP 和 SHC 的检测率。使用荷兰 HIV 监测基金会(Dutch HIV Monitoring Foundation)相对于人群的新 HIV 诊断数据(2015-2019 年)来评估 HIV 发病率。
所有居民的总体 HIV 检测比例为 1.14%,从≥40 岁人群的 0.41%到安的列斯群岛居民的 4.70%不等。总体而言,GP 的检测率普遍高于 SHC 的检测率,总体比率比(RR)为 1.61(95%CI:1.56-1.65),但 15-24 岁人群除外(RR:0.81,95%CI:0.74-0.88)。观察到不同地理区域的 HIV 检测率(每 1000 名居民 1.36 至 39.47 次)和 GP-SHC 比值(RR:0.23 至 7.24)存在较大差异。离 SHC 越远的地区,GP 在 HIV 检测中的作用越大。一般而言,接受检测相对较多的人群也是诊断和发病率最高的人群(例如,男男性行为者,非西方人群)。总体发病率为每 100,000 名居民 10.55 例,从异性恋男性/女性的 3.09 例到 25-29 岁人群的 24.04 例不等。
在远离 SHC 的欠发达地区以及某些人群中,GP 在 HIV 检测中发挥着关键作用。相对较高的发病率通常伴随着相对较高的检测率。已经为移民、受教育程度较低的人、欠发达地区和远离 GP/SHC 的地区找到了改善 HIV 检测的机会。策略包括通过 SHC 分支机构位置和外展活动等方式进行有针对性的额外检测。