Graduate School of Health, Faculty of Health, University of Technology Sydney, Sydney, Australia.
Stakeholder with living experience of acquired brain injury, Sydney, Australia.
J Med Internet Res. 2023 Sep 19;25:e46396. doi: 10.2196/46396.
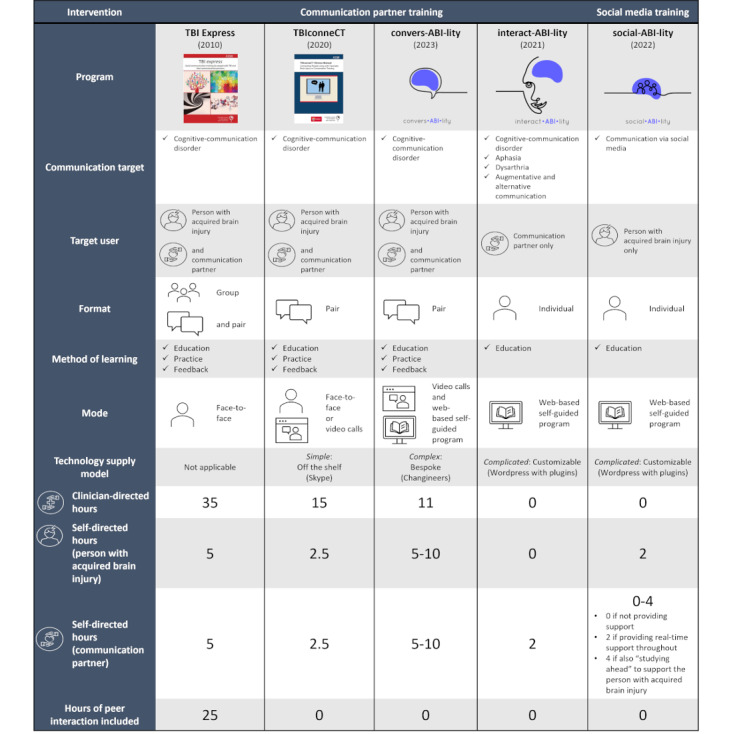
Acquired brain injuries (ABIs), such as stroke and traumatic brain injury, commonly cause cognitive-communication disorders, in which underlying cognitive difficulties also impair communication. As communication is an exchange with others, close others such as family and friends also experience the impact of cognitive-communication impairment. It is therefore an internationally recommended best practice for speech-language pathologists to provide communication support to both people with ABI and the people who communicate with them. Current research also identifies a need for neurorehabilitation professionals to support digital communication, such as social media use, after ABI. However, with >135 million people worldwide affected by ABI, alternate and supplementary service delivery models are needed to meet these communication needs. The "Social Brain Toolkit" is a novel suite of 3 interventions to deliver communication rehabilitation via the internet. However, digital health implementation is complex, and minimal guidance exists for ABI.
This study aimed to support the implementation of the Social Brain Toolkit by coproducing implementation knowledge with people with ABI, people who communicate with people with ABI, clinicians, and leaders in digital health implementation.
A maximum variation sample (N=35) of individuals with living experience of ABI, close others, clinicians, and digital health implementation leaders participated in an explanatory sequential mixed methods design. Stakeholders quantitatively prioritized 4 of the 7 theoretical domains of the Nonadoption, Abandonment, Scale-up, Spread, and Sustainability (NASSS) framework as being the most important for Social Brain Toolkit implementation. Qualitative interview and focus group data collection focused on these 4 domains. Data were deductively analyzed against the NASSS framework with stakeholder coauthors to determine implementation considerations and strategies. A collaborative autoethnography of the research was conducted. Interrelationships between considerations and strategies were identified through a post hoc network analysis.
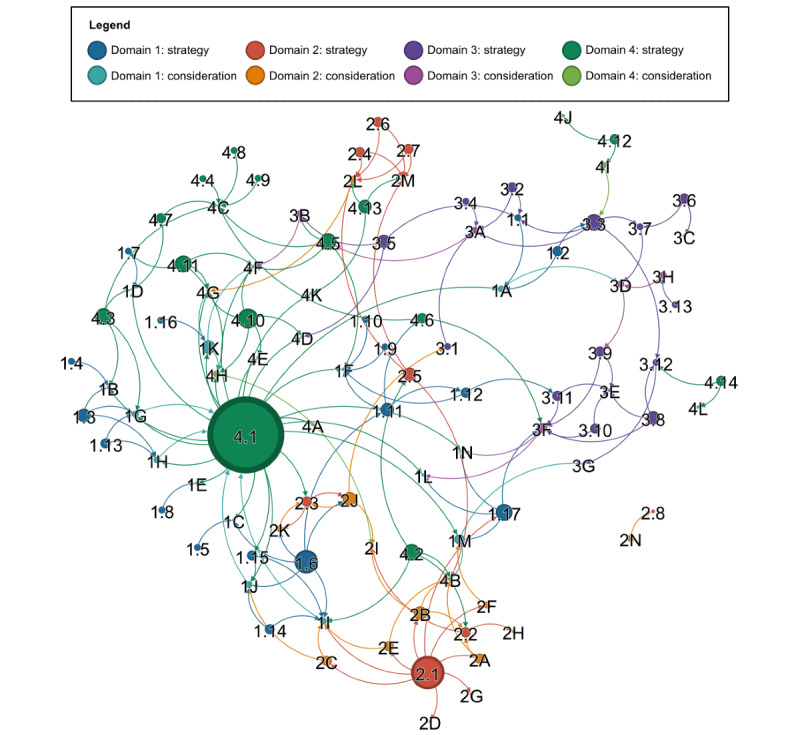
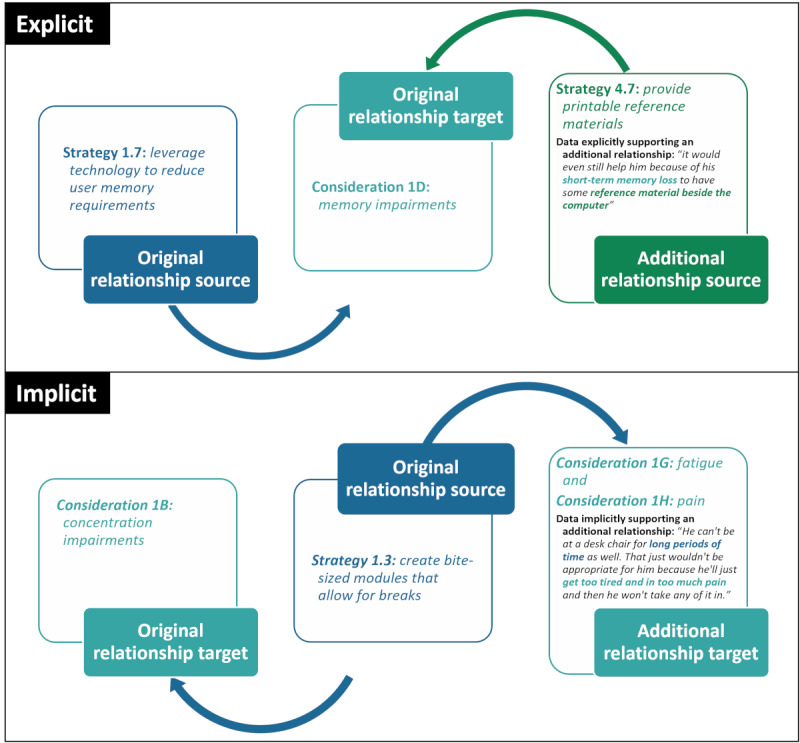
Across the 4 prioritized domains of "condition," "technology," "value proposition," and "adopters," 48 digital health implementation considerations and 52 tailored developer and clinician implementation strategies were generated. Benefits and challenges of coproduction were identified. The post hoc network analysis revealed 172 unique relationships between the identified implementation considerations and strategies, with user and persona testing and responsive design identified as the potentially most impactful strategies.
People with ABI, close others, clinicians, and digital health leaders coproduced new knowledge of digital health implementation considerations for adults with ABI and the people who communicate with them, as well as tailored implementation strategies. Complexity-informed network analyses offered a data-driven method to identify the 2 most potentially impactful strategies. Although the study was limited by a focus on 4 NASSS domains and the underrepresentation of certain demographics, the wealth of actionable implementation knowledge produced supports future coproduction of implementation research with mutually beneficial outcomes for stakeholders and researchers.
INTERNATIONAL REGISTERED REPORT IDENTIFIER (IRRID): RR2-10.2196/35080.
获得性脑损伤(ABI),如中风和创伤性脑损伤,通常会导致认知-交流障碍,其中潜在的认知困难也会损害交流。由于交流是与他人的交流,因此亲密的人,如家人和朋友,也会体验到认知-交流障碍的影响。因此,言语治疗师向 ABI 患者和与他们交流的人提供沟通支持是国际上推荐的最佳实践。目前的研究还确定神经康复专业人员需要支持 ABI 后的数字沟通,例如社交媒体的使用。然而,全球有超过 1.35 亿人受到 ABI 的影响,需要替代和补充服务交付模式来满足这些沟通需求。“社交大脑工具包”是一套通过互联网提供沟通康复的新干预措施。然而,数字健康的实施非常复杂,ABI 方面的指导很少。
本研究旨在通过与 ABI 患者、与 ABI 患者交流的人、临床医生和数字健康实施领导者共同产生实施知识,来支持社交大脑工具包的实施。
具有 ABI 生活经验、亲密他人、临床医生和数字健康实施领导者的最大变异样本(N=35)参与了解释性顺序混合方法设计。利益相关者对非采用、放弃、扩展、传播和可持续性(NASSS)框架的 7 个理论领域中的 4 个进行了定量优先级排序,认为这些领域对社交大脑工具包的实施最重要。定性访谈和焦点小组数据收集集中在这 4 个领域。通过与利益相关者共同作者对 NASSS 框架进行演绎分析,确定了实施考虑因素和策略。对研究进行了合作自传。通过事后网络分析确定了考虑因素和策略之间的相互关系。
在“条件”、“技术”、“价值主张”和“采用者”这 4 个优先领域中,共提出了 48 个数字健康实施考虑因素和 52 个针对开发者和临床医生的定制实施策略。确定了共同生产的好处和挑战。事后网络分析显示,在确定的实施考虑因素和策略之间存在 172 个独特的关系,用户和角色测试以及响应式设计被确定为潜在的最具影响力的策略。
ABI 患者、亲密的人、临床医生和数字健康领导者共同制定了关于 ABI 患者及其交流者的数字健康实施考虑因素以及定制实施策略的新知识。信息丰富的网络分析提供了一种数据驱动的方法来确定最具潜在影响力的 2 个策略。尽管该研究仅限于 4 个 NASSS 领域的重点和某些人群的代表性不足,但产生的大量可操作的实施知识支持了未来与利益相关者和研究人员互惠互利的实施研究的共同生产。
国际注册报告标识符(IRRID):RR2-10.2196/35080。