Medical Intensive Care Unit, University Hospital of Grenoble Alpes, 10217 38043, Grenoble, CS, France.
Grenoble Alpes University, INSERM 1300, HP2, Grenoble, France.
Crit Care. 2023 Sep 19;27(1):359. doi: 10.1186/s13054-023-04631-2.
Non-ventilator-associated ICU-acquired pneumonia (NV-ICU-AP), a nosocomial pneumonia that is not related to invasive mechanical ventilation (IMV), has been less studied than ventilator-associated pneumonia, and never in the context of patients in an ICU for severe acute exacerbation of chronic obstructive pulmonary disease (AECOPD), a common cause of ICU admission. This study aimed to determine the factors associated with NV-ICU-AP occurrence and assess the association between NV-ICU-AP and the outcomes of these patients.
Data were extracted from the French ICU database, OutcomeRea™. Using survival analyses with competing risk management, we sought the factors associated with the occurrence of NV-ICU-AP. Then we assessed the association between NV-ICU-AP and mortality, intubation rates, and length of stay in the ICU.
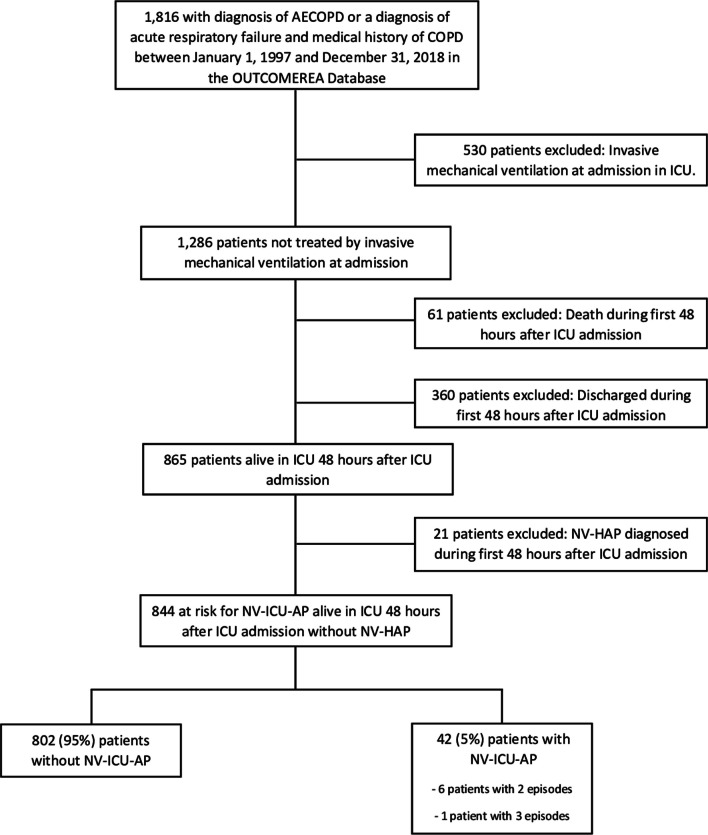
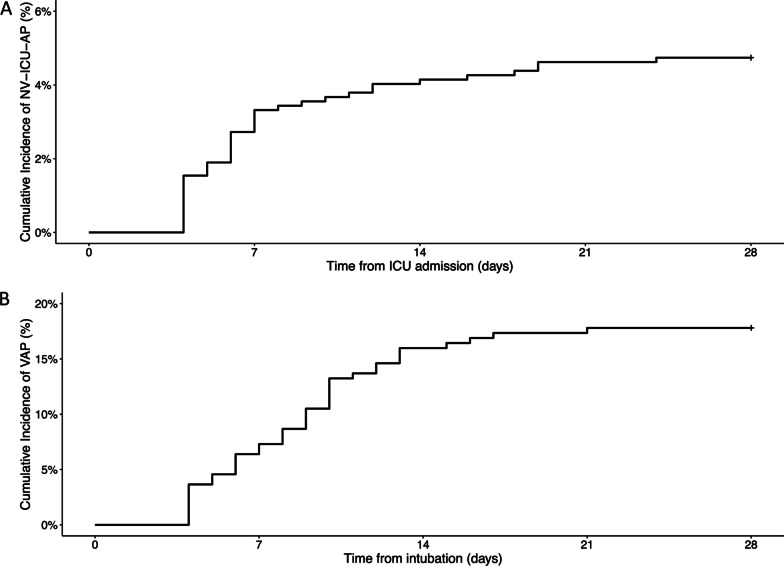
Of the 844 COPD exacerbations managed in ICUs without immediate IMV, NV-ICU-AP occurred in 42 patients (5%) with an incidence density of 10.8 per 1,000 patient-days. In multivariate analysis, prescription of antibiotics at ICU admission (sHR, 0.45 [0.23; 0.86], p = 0.02) and no decrease in consciousness (sHR, 0.35 [0.16; 0.76]; p < 0.01) were associated with a lower risk of NV-ICU-AP. After adjusting for confounders, NV-ICU-AP was associated with increased 28-day mortality (HR = 3.03 [1.36; 6.73]; p < 0.01), an increased risk of intubation (csHR, 5.00 [2.54; 9.85]; p < 0.01) and with a 10-day increase in ICU length of stay (p < 0.01).
We found that NV-ICU-AP incidence reached 10.8/1000 patient-days and was associated with increased risks of intubation, 28-day mortality, and longer stay for patients admitted with AECOPD.
非呼吸机相关性 ICU 获得性肺炎(NV-ICU-AP)是一种与有创机械通气(IMV)无关的医院获得性肺炎,其研究不如呼吸机相关性肺炎多,且从未在因慢性阻塞性肺疾病急性加重(AECOPD)而入住 ICU 的患者中进行过研究,AECOPD 是 ICU 收治的常见原因。本研究旨在确定 NV-ICU-AP 发生的相关因素,并评估 NV-ICU-AP 与这些患者结局的关系。
数据取自法国 ICU 数据库 OutcomeReaTM。我们采用竞争风险管理的生存分析,寻找与 NV-ICU-AP 发生相关的因素。然后,我们评估了 NV-ICU-AP 与死亡率、插管率和 ICU 住院时间的关系。
在 844 例未立即接受 IMV 的 COPD 加重患者中,42 例(5%)发生 NV-ICU-AP,发生率密度为 10.8/1000 患者日。多变量分析显示,入住 ICU 时即开始使用抗生素(校正后 HR,0.45 [0.23;0.86],p=0.02)和意识未减退(校正后 HR,0.35 [0.16;0.76];p<0.01)与 NV-ICU-AP 的风险较低相关。在调整混杂因素后,NV-ICU-AP 与 28 天死亡率增加(HR=3.03 [1.36;6.73];p<0.01)、插管风险增加(校正后 csHR,5.00 [2.54;9.85];p<0.01)和 ICU 住院时间延长 10 天(p<0.01)相关。
我们发现 NV-ICU-AP 的发生率为 10.8/1000 患者日,与 AECOPD 患者的插管、28 天死亡率和 ICU 住院时间延长风险增加相关。