Riley E Leonard, Brunson J Cory, Eydgahi Soroush, Brantly Mark L, Lascano Jorge E
Department of Internal Medicine, Division of Pulmonary, Critical Care, and Sleep Medicine, Kansas City Veterans Affairs Medical Center, Kansas City, MO, USA.
Laboratory for Systems Medicine, Division of Pulmonary, Critical Care, and Sleep Medicine, University of Florida College of Medicine, Gainesville, FL, USA.
ERJ Open Res. 2023 Sep 18;9(5). doi: 10.1183/23120541.00302-2023. eCollection 2023 Sep.
Alpha-1 antitrypsin deficiency (AATD) is an under-recognised genetic cause of chronic obstructive lung disease, and many fewer cases than estimated have been identified. Can a reported respiratory and hepatic disease history from a large AATD testing database be used to stratify a person's risk of severe AATD?
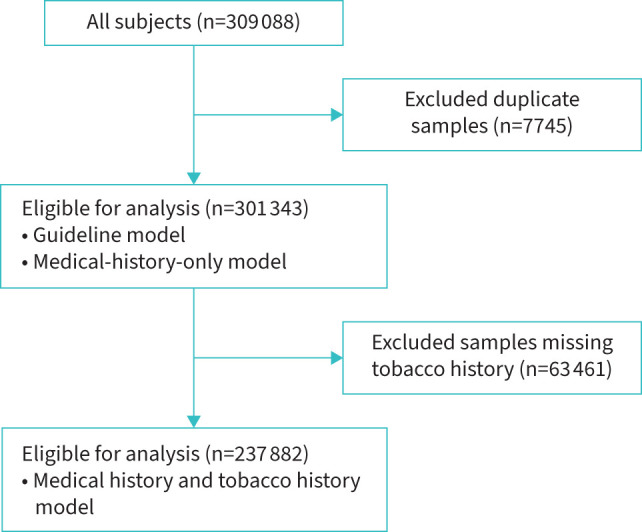
We analysed data extracted from the AATD National Detection Program. Demographics and medical history were evaluated to predict AATD PI*ZZ genotype. Logistic regression and integer programming models identified predictors and obtained risk scores. These were internally validated on a subset of the data.
Out of 301 343 subjects, 1529 (0.5%) had PI*ZZ genotype. Predictors of severe AATD were asthma, bronchitis, emphysema, allergies, bronchiectasis, family history of AATD, cirrhosis, hepatitis and history of abnormal liver function tests. The derived model establishes a subject's risk of severe AATD, and scores ≥0 had an estimated risk of 0.41%, sensitivity 84.62% and specificity 24.32%. A model simulating guideline recommendations had an estimated risk of 0.51% with a sensitivity of 37.98% and specificity 46.60%. By recommending screening for scores ≥0, we estimate that more subjects would be screened (75.7% 53.4%) and detected (84.6% 58.2%) compared to a guideline-simulated model.
This medical history risk model is a useful predictive tool to detect subjects at greater risk of having severe AATD and improves sensitivity of detection. Scores <0 are at lower risk and may need not be screened; testing is recommended for scores ≥0 and consistent with current guidelines.
α-1抗胰蛋白酶缺乏症(AATD)是慢性阻塞性肺疾病一个未得到充分认识的遗传病因,已确诊的病例数比预估的要少得多。能否根据一个大型AATD检测数据库中报告的呼吸和肝脏疾病史来分层个体患严重AATD的风险?
我们分析了从AATD国家检测项目中提取的数据。评估人口统计学和病史以预测AATD PI*ZZ基因型。逻辑回归和整数规划模型确定了预测因素并获得风险评分。这些在数据子集上进行了内部验证。
在301343名受试者中,1529名(0.5%)具有PI*ZZ基因型。严重AATD的预测因素包括哮喘、支气管炎、肺气肿、过敏、支气管扩张、AATD家族史、肝硬化、肝炎以及肝功能检查异常史。推导的模型确定了个体患严重AATD的风险,评分≥0的个体估计风险为0.41%,敏感性为84.62%,特异性为24.32%。一个模拟指南建议的模型估计风险为0.51%,敏感性为37.98%,特异性为46.60%。通过建议对评分≥0的个体进行筛查,我们估计与模拟指南的模型相比,将有更多的个体接受筛查(75.7% 对53.4%)和被检测出(84.6% 对58.2%)。
这种病史风险模型是一种有用的预测工具,可用于检测患严重AATD风险较高的个体,并提高检测的敏感性。评分<0的个体风险较低,可能无需筛查;建议对评分≥0的个体进行检测,这与当前指南一致。