Department of Health Services Research, Management & Policy, College of Public Health & Health Professions, University of Florida, Gainesville, FL, USA.
Department of Speech, Language, and Hearing Sciences, University of Florida, Gainesville, FL, USA.
Womens Health (Lond). 2023 Jan-Dec;19:17455057231199061. doi: 10.1177/17455057231199061.
Black Americans have a higher prevalence of stroke and stroke-related deaths than any other racial group. Racial disparities in stroke outcomes are even wider among women than men. Conventional studies have cited differences in lifestyle (i.e. smoking, alcohol consumption, etc.) and vascular risk factors between races as the source of these disparities. However, these studies fail to account for the higher prevalence of minoritized populations at the lower end of the socioeconomic distribution.
This study explores differences in stroke risk factors across age and socioeconomic cohorts to determine whether comorbidities can sufficiently explain disparities at all ages and income levels.
Using the 2006-2018 National Health Interview Survey data, statistical analysis evaluated differences in risk factors among a full sample cohort (aged 18-85 years; = 131,091) and a "young" subsample cohort (aged 18-59 years; = 6183) of women.
Logistics and unconditional quantile regression models assessed the relationship between stroke and comorbid, demographic, and behavioral characteristics across socioeconomic classes.
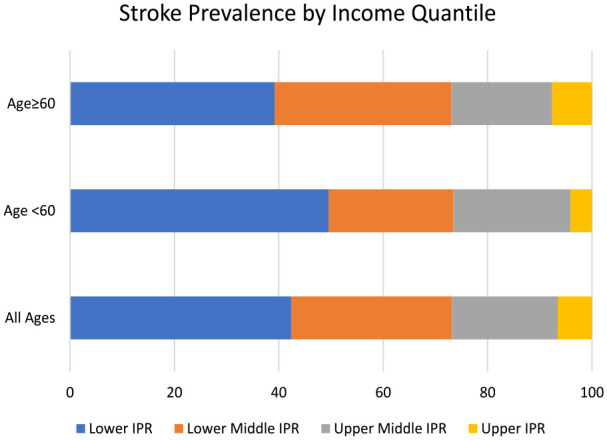
Results suggest that Black women had a 1.415-fold (confidence interval = 1.259, 1.591) higher likelihood of stroke compared with White women after controlling for age, behavior, and comorbidities. Racial disparities were not statistically significant at the higher income ranges for either the full (odds ratio = 1.404, = 0.3114) or young samples (odds ratio = 1.576, = 0.7718). However, Blacks had significantly higher odds of stroke in the lower quartiles (lower odds ratio: 1.329, = 0.0242; lower middle odds ratio: 1.233, = 0.0486; and upper middle odds ratio: 1.994, = 0.0005). Disparities were larger among young women (odds ratio = 1.449, confidence interval = 1.211, 1.734).
While comorbidities were highly associated with stroke prevalence in all socioeconomic cohorts, Blacks only had higher relative odds in the lower income classes. Lack of biological or behavioral explanations for these findings suggests that unobserved or uncontrolled factors such as systemic racism, prejudicial institutions, or differential treatment may contribute to this.
非裔美国人患中风和中风相关死亡的比例高于任何其他种族群体。在女性中,中风结果的种族差异甚至比男性更大。传统研究认为,种族之间生活方式(例如吸烟、饮酒等)和血管风险因素的差异是造成这些差异的原因。然而,这些研究没有考虑到处于社会经济分布低端的少数群体的更高患病率。
本研究探讨了不同年龄和社会经济群体中风风险因素的差异,以确定是否合并症可以充分解释所有年龄和收入水平的差异。
使用 2006-2018 年全国健康访谈调查数据,统计分析评估了全样本队列(年龄 18-85 岁;n=131091)和“年轻”子样本队列(年龄 18-59 岁;n=6183)中女性中风风险因素之间的差异。
逻辑回归和无条件分位数回归模型评估了中风与合并症、人口统计学和行为特征之间的关系,跨越社会经济阶层。
结果表明,在控制年龄、行为和合并症后,与白人女性相比,黑人女性中风的可能性高 1.415 倍(置信区间 1.259,1.591)。对于全样本(比值比 1.404,p=0.3114)或年轻样本(比值比 1.576,p=0.7718),收入较高的种族差异在统计学上不显著。然而,黑人在较低四分位数中风的可能性明显更高(较低比值比:1.329,p=0.0242;较低中值比值比:1.233,p=0.0486;较高中值比值比:1.994,p=0.0005)。年轻女性的差异更大(比值比 1.449,置信区间 1.211,1.734)。
虽然合并症与所有社会经济群体的中风患病率高度相关,但只有在较低的收入群体中,黑人的相对优势更高。对于这些发现,没有生物学或行为学的解释表明,未观察到或未控制的因素,如系统性种族主义、偏见机构或差异待遇,可能是造成这种情况的原因。