Xie Charlies L, Whitman Gary J, Middleton Lavinia P, Bevers Therese B, Bedrosian Isabelle, Chung Hannah L
MD Anderson Cancer Center, Department of Breast Imaging, Houston, TX, USA.
MD Anderson Cancer Center, Department of Pathology, Houston, TX, USA.
J Breast Imaging. 2023 Jul 22;5(5):575-584. doi: 10.1093/jbi/wbad049. eCollection 2023 Sep-Oct.
To compare flat epithelial atypia (FEA) upgrade rates after excision versus surveillance and to identify variables associated with upgrade.
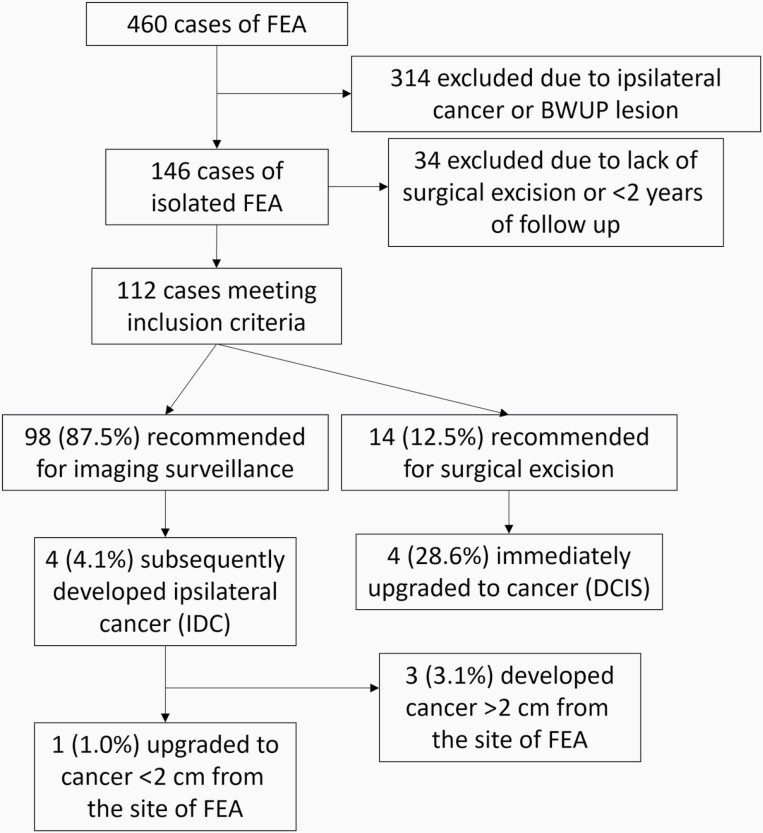
This single-institution retrospective study identified isolated FEA cases determined by percutaneous biopsy from April 2005 through July 2022 with excision or ≥2 years surveillance. All cases were recommended for excision or surveillance based on multidisciplinary discussion of clinical, imaging, and pathologic variables with emphasis on sampling adequacy and significant atypia. Truth was determined by pathology at excision or the absence of cancer on surveillance. Upgrade was defined as cancer occurring ≤2 cm from the biopsy site. Demographic, imaging, and biopsy variables were compared between those that did and did not upgrade.
Among 112 cases of isolated FEA, imaging findings included calcifications in 81.3% (91/112), MRI lesions in 11.6% (13/112), and distortions or masses in 7.1% (8/112). Excision was recommended in 12.5% (14/112) and surveillance in 87.5% (98/112) of cases. Among those recommended for excision, 28.6% (4/14) of cases were upgraded, all to ductal carcinoma in situ. In those recommended for surveillance, 1.0% (1/98) were upgraded to invasive cancer. Overall, FEA had a 4.5% (5/112) upgrade rate, and 2.7% (3/112) also developed cancer >2 cm from the FEA. There were no significant differences in demographic, imaging, and biopsy variables between those that did and did not upgrade to cancer.
Multidisciplinary management of isolated FEA distinguishes those at higher risk of upgrade to cancer (28.6%) in whom surgery is warranted from those at low risk of upgrade (1.0%) who can be managed non-operatively.
比较切除术后与监测后的扁平上皮异型增生(FEA)升级率,并确定与升级相关的变量。
这项单机构回顾性研究确定了2005年4月至2022年7月期间经皮活检确诊的孤立性FEA病例,这些病例接受了切除或至少2年的监测。所有病例均根据临床、影像学和病理变量的多学科讨论建议进行切除或监测,重点是取样充分性和显著异型性。通过切除时的病理检查或监测时未发现癌症来确定实际情况。升级定义为在活检部位≤2 cm处发生癌症。对升级和未升级的患者的人口统计学、影像学和活检变量进行比较。
在112例孤立性FEA病例中,影像学表现包括钙化81.3%(91/112)、MRI病变11.6%(13/112)、变形或肿块7.1%(8/112)。12.5%(14/112)的病例建议切除,87.5%(98/112)的病例建议监测。在建议切除的病例中,28.6%(4/14)升级,均为导管原位癌。在建议监测的病例中,1.0%(1/98)升级为浸润性癌。总体而言,FEA的升级率为4.5%(5/112),2.7%(3/112)在距FEA >2 cm处也发生了癌症。升级和未升级为癌症的患者在人口统计学、影像学和活检变量方面无显著差异。
孤立性FEA的多学科管理区分了升级为癌症风险较高(28.6%)且需要手术的患者与升级风险较低(1.0%)且可进行非手术管理的患者。