Miletínová E, Piorecký M, Koudelka V, Jiříček S, Tomeček D, Brunovský M, Horáček J, Bušková J
National Institute of Mental Health, Topolova 748, Klecany, Czech Republic.
Third Faculty of Medicine, Charles University in Prague, Ruská 87, Prague, Czech Republic.
Sleep Med X. 2023 Sep 14;6:100086. doi: 10.1016/j.sleepx.2023.100086. eCollection 2023 Dec 15.
NREM parasomnias also known as disorders of arousal (DOA) are characterised by abnormal motor and autonomic activation during arousals primarily from slow wave sleep. Dissociative state between sleep and wake is likely responsible for clinical symptoms of DOA. We therefore investigated potential dissociation outside of parasomnic events by using simultaneous 256-channel EEG (hdEEG) and functional magnetic resonance imaging (fMRI).
Eight DOA patients (3 women, mean age = 27.8; SD = 4.2) and 8 gender and age matched healthy volunteers (3 women, mean age = 26,5; SD = 4.0) were included into the study. They underwent 30-32 h of sleep deprivation followed by hdEEG and fMRI recording. We determined 2 conditions: falling asleep (FA) and arousal (A), that occurred outside of deep sleep and/or parasomnic event. We used multimodal approach using data obtained from EEG, fMRI and EEG-fMRI integration approach.
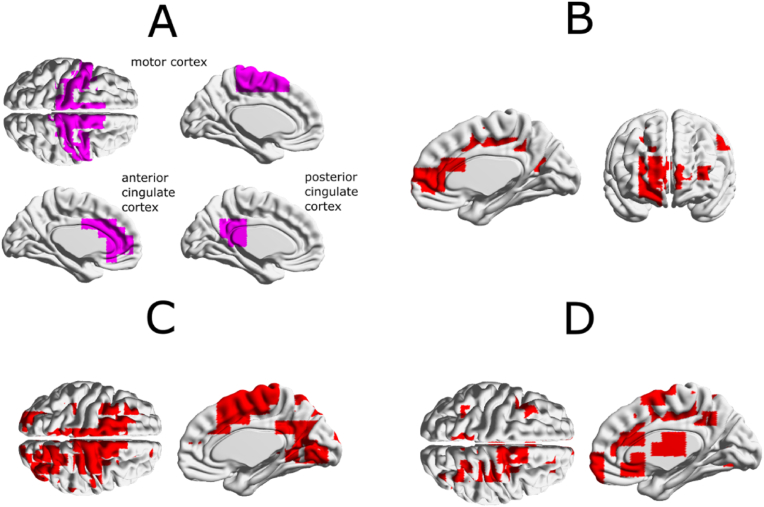
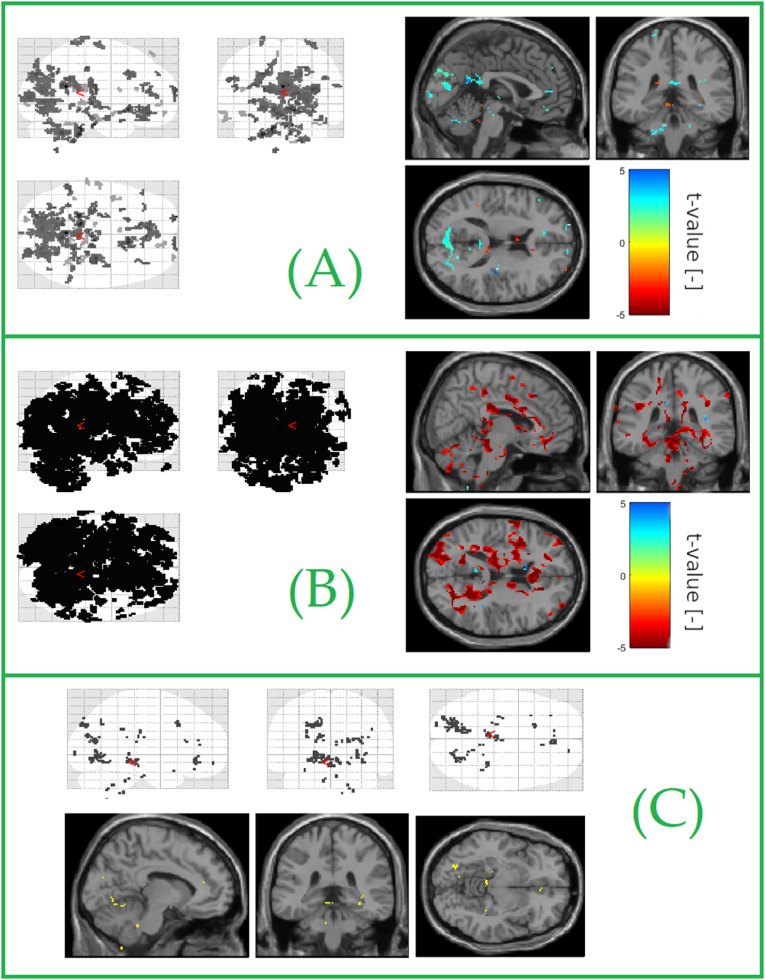
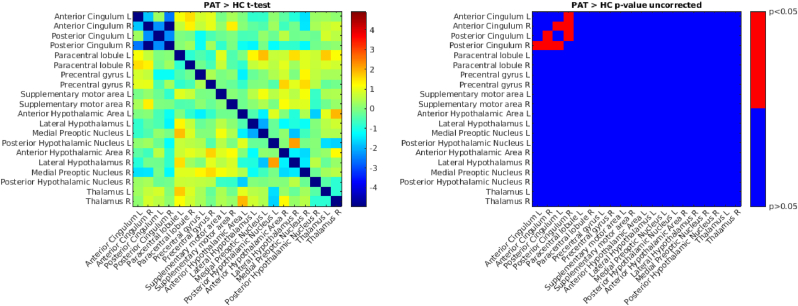
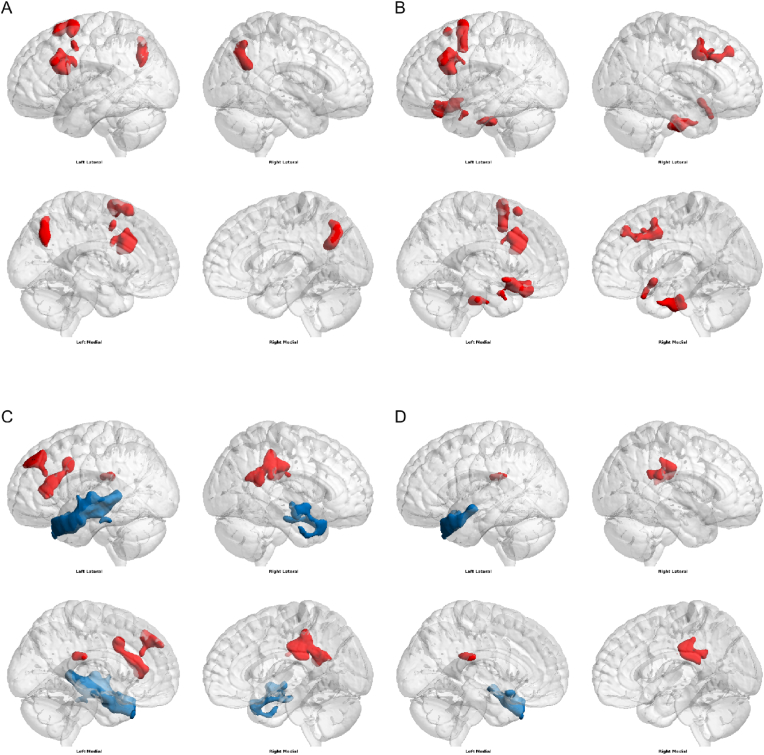
DOA patients showed increase in delta and beta activity over postcentral gyrus and cuneus during awakening period. This group expressed increased connectivity between motor cortex and cingulate during arousals unrelated to parasomnic events in the beta frequency band. They also showed lower connectivity between different portions of cingulum. In contrast, the greater connectivity was found between thalamus and some cortical areas, such as occipital cortex.
Our findings suggest a complex alteration in falling asleep and arousal mechanisms at both subcortical and cortical levels in response to sleep deprivation. As this alteration is present also outside of slow wave sleep and/or parasomnic episodes we believe this could be a trait factor of DOA.
非快速眼动睡眠期异态睡眠也称为觉醒障碍(DOA),其特征是主要从慢波睡眠中觉醒时出现异常的运动和自主神经激活。睡眠与觉醒之间的分离状态可能是DOA临床症状的原因。因此,我们通过同步256通道脑电图(高清脑电图,hdEEG)和功能磁共振成像(fMRI)研究了异态睡眠事件之外的潜在分离情况。
8名DOA患者(3名女性,平均年龄 = 27.8岁;标准差 = 4.2)和8名年龄及性别匹配的健康志愿者(3名女性,平均年龄 = 26.5岁;标准差 = 4.0)纳入本研究。他们经历了30 - 32小时的睡眠剥夺,随后进行高清脑电图和功能磁共振成像记录。我们确定了2种情况:入睡(FA)和觉醒(A),这些情况发生在深度睡眠和/或异态睡眠事件之外。我们采用了多模态方法,使用从脑电图、功能磁共振成像以及脑电图 - 功能磁共振成像整合方法获得的数据。
DOA患者在觉醒期中央后回和楔叶的δ波和β波活动增加。该组在与异态睡眠事件无关的觉醒期间,β频段的运动皮层和扣带回之间的连接性增加。他们还显示扣带不同部分之间的连接性较低。相比之下,丘脑与一些皮层区域,如枕叶皮层之间的连接性更强。
我们的研究结果表明,在睡眠剥夺的情况下,皮层下和皮层水平的入睡和觉醒机制存在复杂改变。由于这种改变也出现在慢波睡眠和/或异态睡眠发作之外,我们认为这可能是DOA的一个特质因素。