Bober Robert M, Milani Richard V, Kachur Sergey M, Morin Daniel P
Department of Cardiovascular Diseases, John Ochsner Heart and Vascular Institute, Ochsner Health, 1514 Jefferson Highway, New Orleans, LA, 70121-2483, USA.
Ochsner Clinical School, Queensland University School of Medicine, New Orleans, LA, USA.
EJNMMI Res. 2023 Sep 27;13(1):87. doi: 10.1186/s13550-023-01037-7.
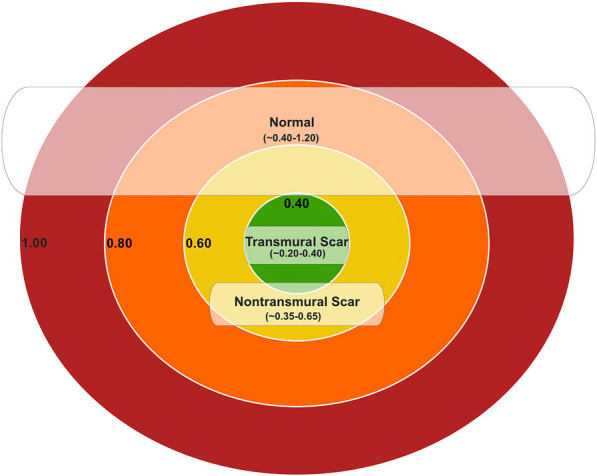
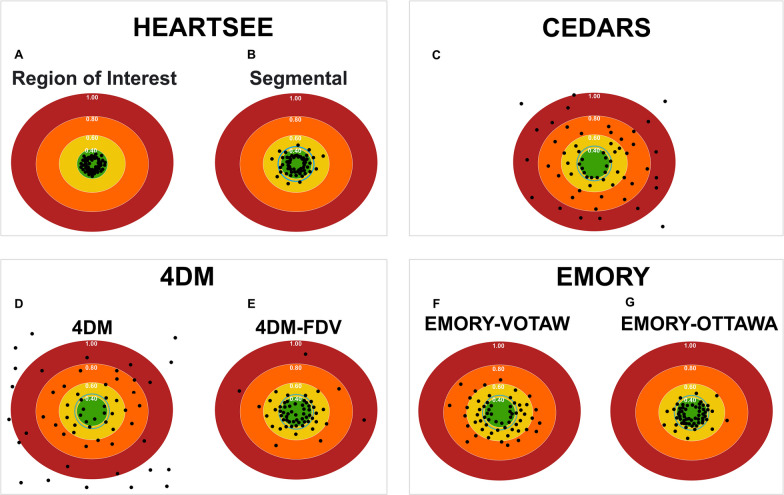
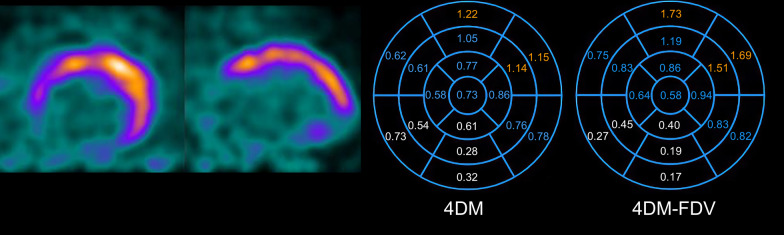
Composite invasive and non-invasive data consistently demonstrate that resting myocardial blood flow (rMBF) in regions of known transmural myocardial scar (TMS) converge on a value of ~ 0.30 mL/min/g or lower. This value has been confirmed using the 3 most common myocardial perfusion agents (N, O-HO and Rb) incorporating various kinetic models on older 2D positron emission tomography (PET) systems. Thus, rMBF in regions of TMS can serve as a reference "truth" to evaluate low-end accuracy of various PET systems and software packages (SWPs). Using Rb on a contemporary 3D-PET-CT system, we sought to determine whether currently available SWP can accurately and precisely measure rMBF in regions of known TMS.
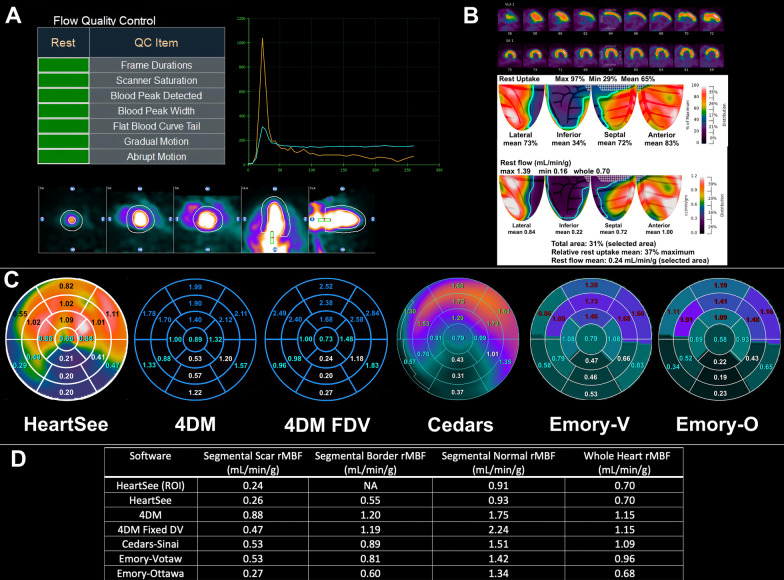
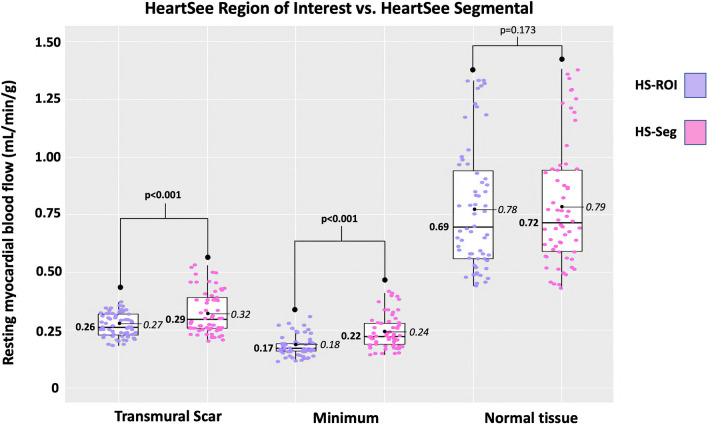
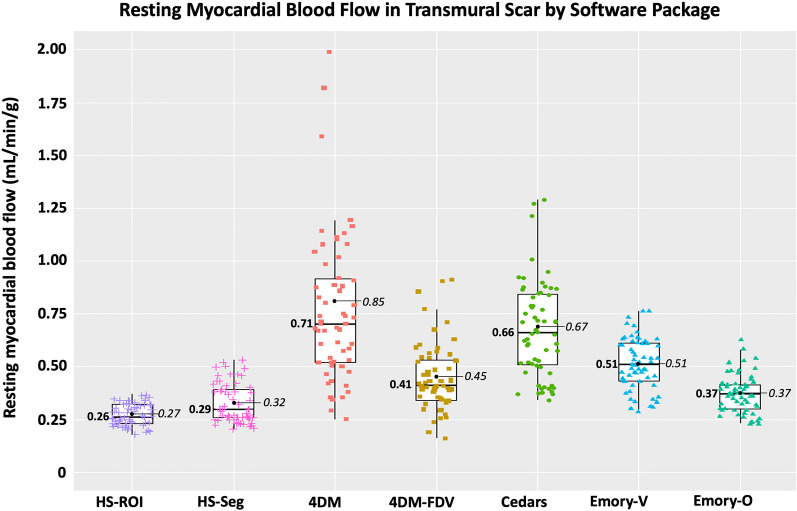
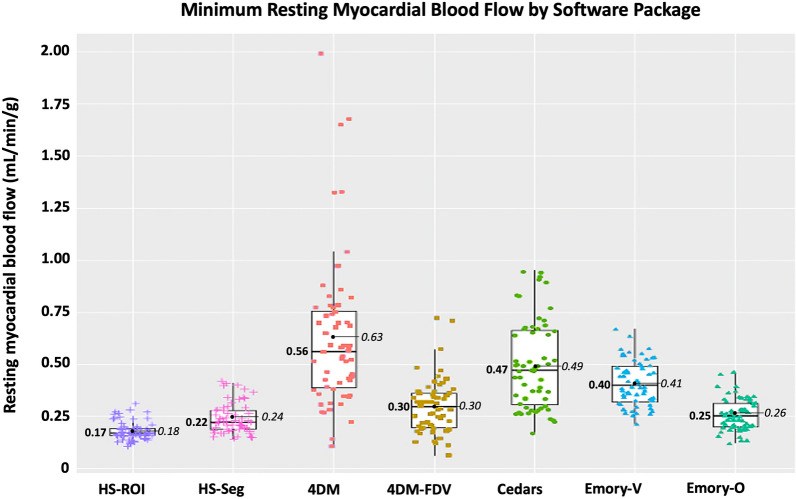
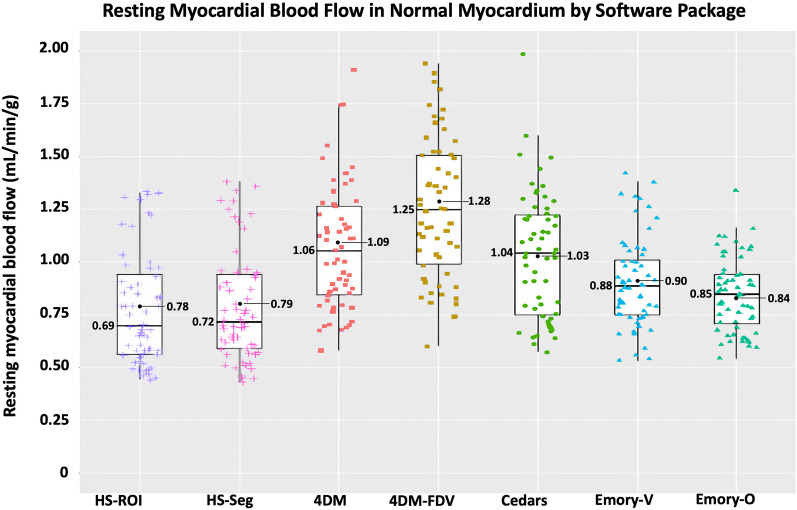
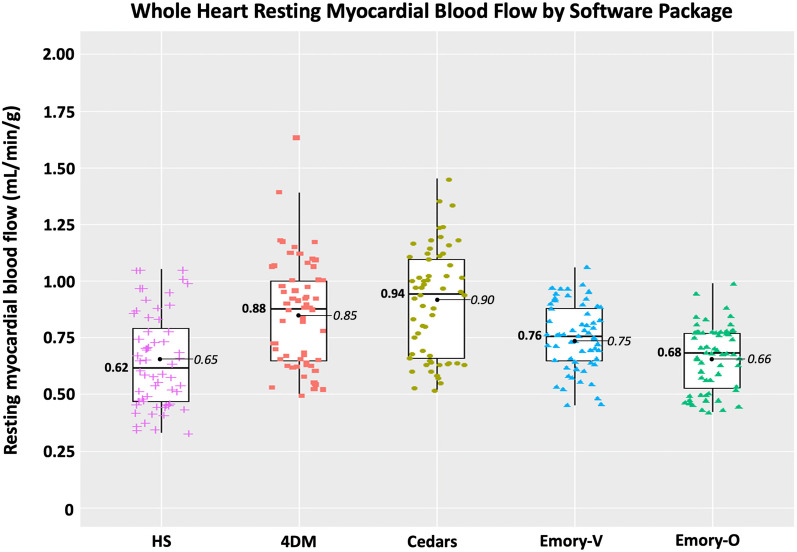
Median rMBF (in mL/min/g) and COV in regions of TMS were 0.71 [IQR 0.52-1.02] and 0.16 with 4DM; 0.41 [0.34-0.54] and 0.10 with 4DM-FVD; 0.66 [0.51-0.85] and 0.11 with Cedars; 0.51 [0.43-0.61] and 0.08 with Emory-Votaw; 0.37 [0.30-0.42], 0.07 with Emory-Ottawa, and 0.26 [0.23-0.32], COV 0.07 with HeartSee.
SWPs varied widely in low end accuracy based on measurement of rMBF in regions of known TMS. 3D PET using Rb and HeartSee software accurately (0.26 mL/min/g, consistent with established values) and precisely (COV = 0.07) quantified rMBF in regions of TMS. The Emory-Ottawa software yielded the next-best accuracy (0.37 mL/min/g), though rMBF was higher than established gold-standard values in ~ 5% of the resting scans. 4DM, 4DM-FDV, Cedars and Emory-Votaw SWP consistently resulted values higher than the established gold standard (0.71, 0.41, 0.66, 0.51 mL/min/g, respectively), with higher interscan variability (0.16, 0.11, 0.11, and 0.09, respectively).
clinicaltrial.gov, NCT05286593, Registered December 28, 2021, https://clinicaltrials.gov/ct2/show/NCT05286593 .
综合侵入性和非侵入性数据一致表明,已知透壁心肌瘢痕(TMS)区域的静息心肌血流量(rMBF)趋于~0.30 mL/min/g或更低的值。使用三种最常见的心肌灌注剂(N、O-HO和Rb)并结合各种动力学模型,在较旧的二维正电子发射断层扫描(PET)系统上已证实了该值。因此,TMS区域的rMBF可作为参考“真值”,以评估各种PET系统和软件包(SWP)的低端准确性。在当代的三维PET-CT系统上使用Rb,我们试图确定当前可用的SWP是否能够准确且精确地测量已知TMS区域的rMBF。
TMS区域的rMBF中位数(以mL/min/g为单位)和变异系数在使用4DM时分别为0.71 [四分位间距0.52 - 1.02]和0.16;使用4DM-FVD时为0.41 [0.34 - 0.54]和0.10;使用Cedars时为0.66 [0.51 - 0.85]和0.11;使用Emory-Votaw时为0.51 [0.43 - 0.61]和0.08;使用Emory-Ottawa时为0.37 [0.30 - 0.42],变异系数为0.07;使用HeartSee时为0.26 [0.23 - 0.32],变异系数为0.07。
基于已知TMS区域rMBF的测量,SWP在低端准确性方面差异很大。使用Rb和HeartSee软件的三维PET准确地(0.26 mL/min/g,与既定值一致)且精确地(变异系数 = 0.07)量化了TMS区域的rMBF。Emory-Ottawa软件的准确性次之(0.37 mL/min/g),尽管在约5%的静息扫描中rMBF高于既定的金标准值。4DM、4DM-FDV、Cedars和Emory-Votaw SWP得出的值始终高于既定的金标准(分别为0.71、0.41、0.66、0.51 mL/min/g),且扫描间变异性更高(分别为0.16、0.11、0.11和0.09)。
clinicaltrial.gov,NCT05286593,于2021年12月28日注册,https://clinicaltrials.gov/ct2/show/NCT05286593 。