Hou Peixian, Wu Dawen, Nie Yan, Wei Hong, Liu Longqian, Yang Guoyuan
Department of Ophthalmology, West China Hospital, Sichuan University, Chengdu, Sichuan, China.
Laboratory of Optometry and Vision Sciences, West China Hospital, Sichuan University, Chengdu, Sichuan, China.
Front Pharmacol. 2023 Sep 11;14:1227787. doi: 10.3389/fphar.2023.1227787. eCollection 2023.
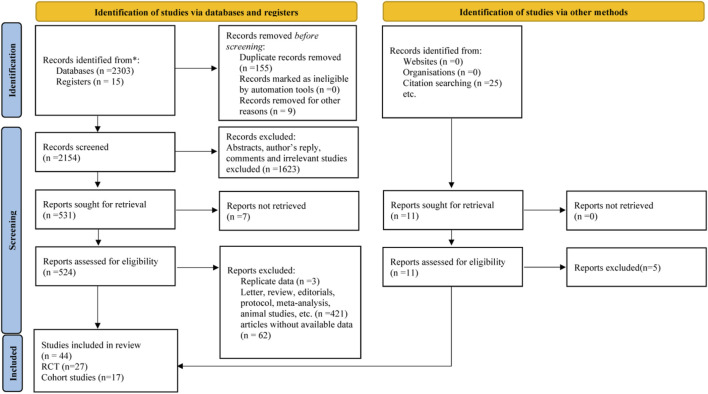
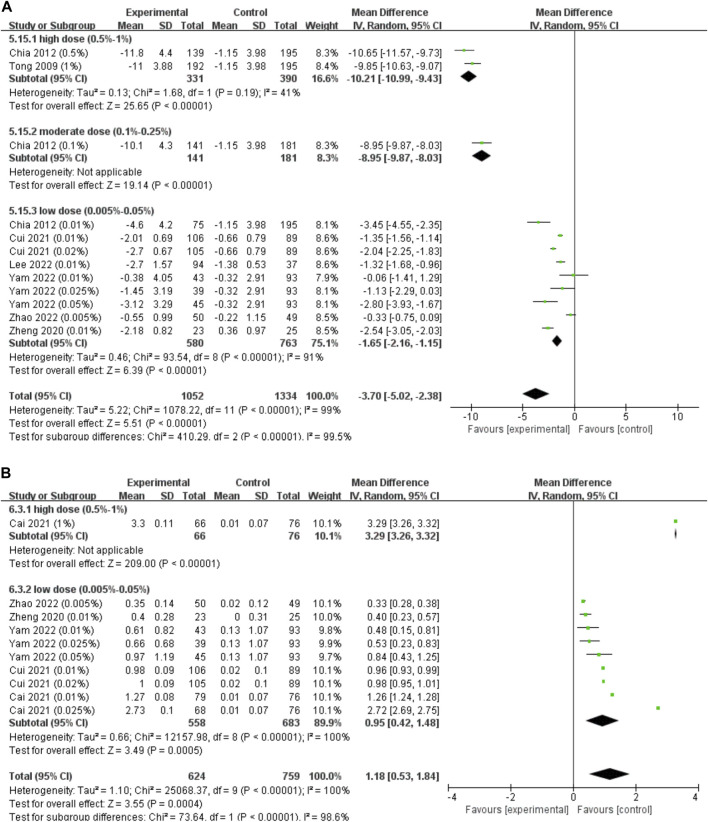
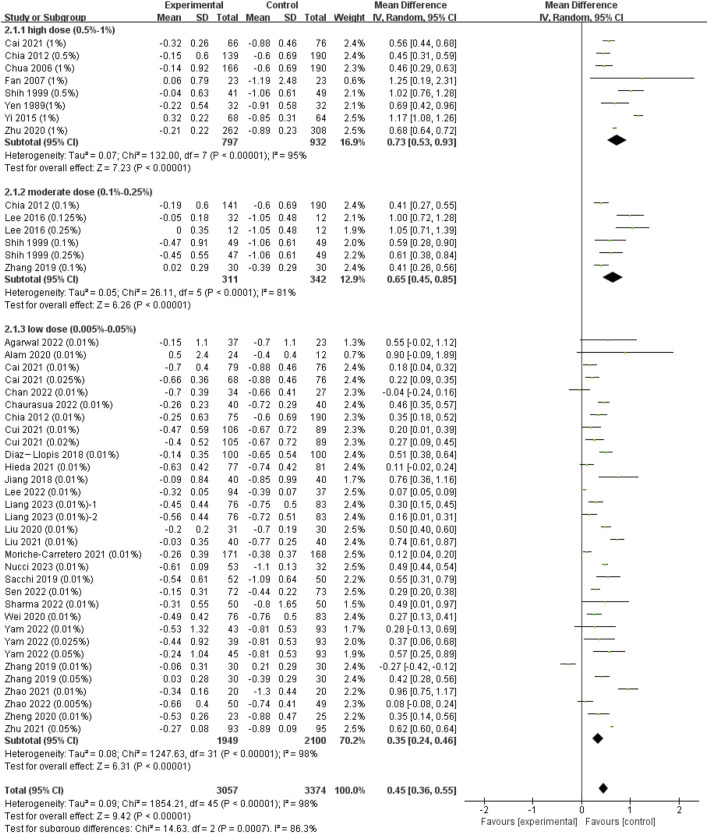
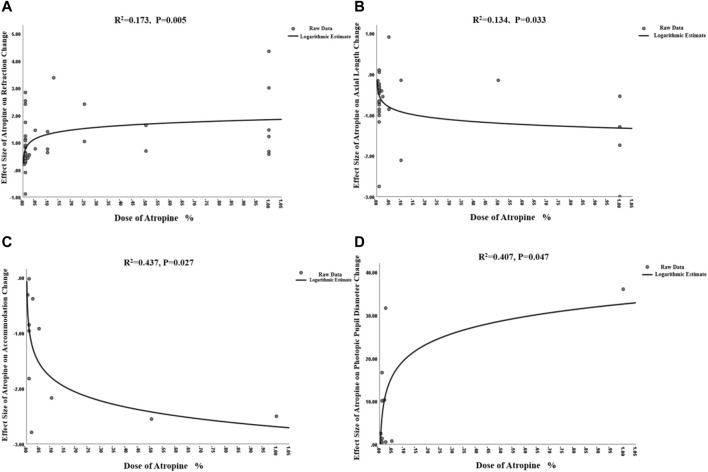
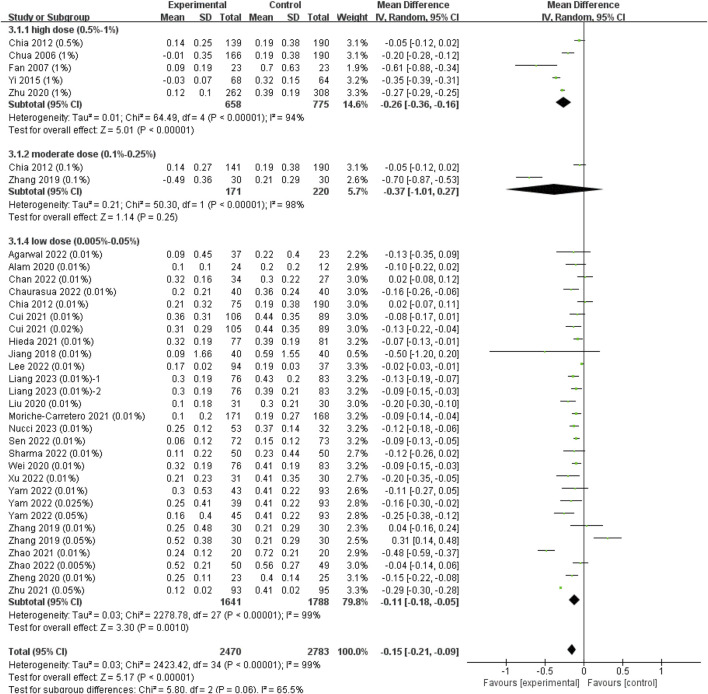
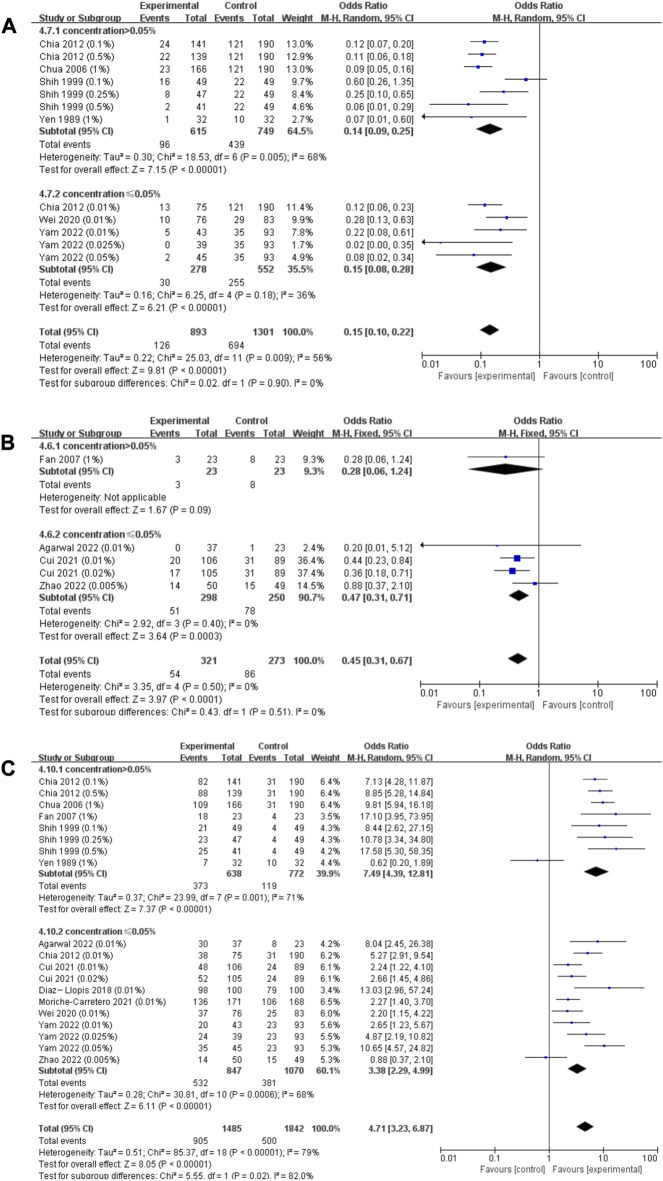
To comprehensively reassess the efficacy and safety of different concentrations of atropine for retarding myopia progression and seek the most appropriate therapeutic concentration for clinical practice. We searched PubMed, Cochrane Library, Embase, Chinese Science and Technology Periodicals (VIP) and China National Knowledege Infrastructure (CNKI) from their inception to 23 March 2023, to obtain eligible randomized controlled trials (RCTs) and cohort studies that had atropine in at least one treatment arm and placebo/no intervention in another arm. We evaluated the risk of bias of the RCTs according to the recommendations of the Cochrane Collaboration for RCTs and quality of cohort studies by the Newcastle‒Ottawa Scale. Weighted mean difference (WMD), 95% confidence interval were calculated for meta-analysis. All data analyses were performed using Review Manager 5.3, STATA 12.0 and SPSS 26.0 software. A total of 44 studies were included in the meta-analysis. Weighted mean difference (WMD) were 0.73 diopters (D), 0.65 D, 0.35 D per year in refraction progression ( = 14.63, = 86.3%; < 0.001) and -0.26 mm, -0.37 mm, -0.11 mm per year in axial length progression ( = 5.80, = 65.5%; = 0.06) for high (0.5%-1%), moderate (0.1%-0.25%), and low (0.005%-0.05%) dose atropine groups, respectively. Logarithmic dose‒response correlations were found between atropine and their effect on change of refraction, axial length, accommodation and photopic pupil diameter. Through these curves, we found that atropine with concentrations ≤0.05% atropine resulted in a residual value of accommodation of more than 5 D and an increase in pupil diameter no more than 3 mm. Higher doses of atropine resulted in a higher incidence of adverse effects, of which the incidence of photophobia was dose-dependent ( = 0.477, = 0.029). Both the efficacy and risk of adverse events for atropine treatment of myopia were mostly dose dependent. Comprehensively considered the myopia control effect and safety of each dose, 0.05% may be the best concentration of atropine to control myopia progression at present, at which myopia is better controlled and the side effects are tolerable. https://www.crd.york.ac.uk/PROSPERO/#recordDetails, CRD42022377705.
为全面重新评估不同浓度阿托品延缓近视进展的疗效和安全性,并寻找临床实践中最合适的治疗浓度。我们检索了PubMed、Cochrane图书馆、Embase、中国科技期刊数据库(维普)和中国知网,检索时间从各数据库建库至2023年3月23日,以获取符合条件的随机对照试验(RCT)和队列研究,这些研究至少有一个治疗组使用阿托品,另一个组使用安慰剂/无干预。我们根据Cochrane协作网对RCT的推荐评估RCT的偏倚风险,并通过纽卡斯尔-渥太华量表评估队列研究的质量。计算加权平均差(WMD)、95%置信区间用于荟萃分析。所有数据分析使用Review Manager 5.3、STATA 12.0和SPSS 26.0软件进行。荟萃分析共纳入44项研究。高剂量(0.5%-1%)、中剂量(0.1%-0.25%)和低剂量(0.005%-0.05%)阿托品组的屈光进展每年加权平均差分别为0.73屈光度(D)、0.65 D、0.35 D(χ² = 14.63,P = 86.3%;P < 0.001),眼轴长度进展每年分别为-0.26 mm、-0.37 mm、-0.11 mm(χ² = 5.80,P = 65.5%;P = 0.06)。发现阿托品与其对屈光、眼轴长度、调节和明视瞳孔直径变化的影响之间存在对数剂量-反应相关性。通过这些曲线,我们发现浓度≤0.05%阿托品导致调节残余值超过5 D,瞳孔直径增加不超过3 mm。更高剂量的阿托品导致不良反应发生率更高,其中畏光发生率呈剂量依赖性(χ² = 0.477,P = 0.029)。阿托品治疗近视的疗效和不良事件风险大多呈剂量依赖性。综合考虑各剂量的近视控制效果和安全性,0.05%可能是目前控制近视进展的最佳阿托品浓度,此时近视得到较好控制且副作用可耐受。https://www.crd.york.ac.uk/PROSPERO/#recordDetails, CRD42022377705