Centre for Cardiovascular Medicine and Devices (D.A.J., A.-M.B., M.K., K.S.R., M.A., L.W., N.F., R.R., A.B., A.A., A.M.), Barts Heart Centre, Barts Health NHS Trust, London, UK.
Barts Cardiovascular Clinical Trials Unit (D.A.J., T.G., A.B., A.A.), Barts Heart Centre, Barts Health NHS Trust, London, UK.
Circulation. 2023 Oct 31;148(18):1371-1380. doi: 10.1161/CIRCULATIONAHA.123.064465. Epub 2023 Sep 29.
Patients with previous coronary artery bypass grafting often require invasive coronary angiography (ICA). However, for these patients, the procedure is technically more challenging and has a higher risk of complications. Observational studies suggest that computed tomography cardiac angiography (CTCA) may facilitate ICA in this group, but this has not been tested in a randomized controlled trial.
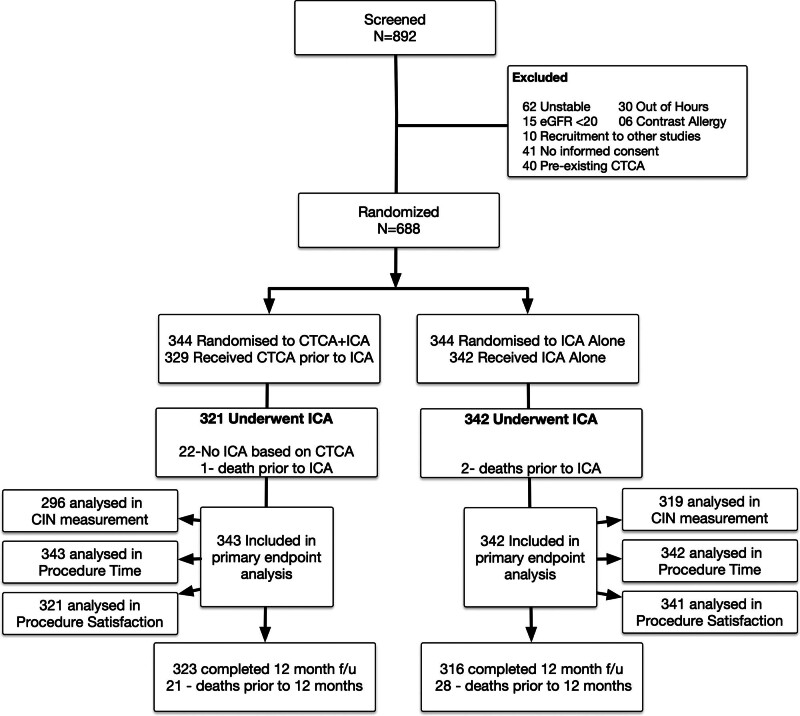
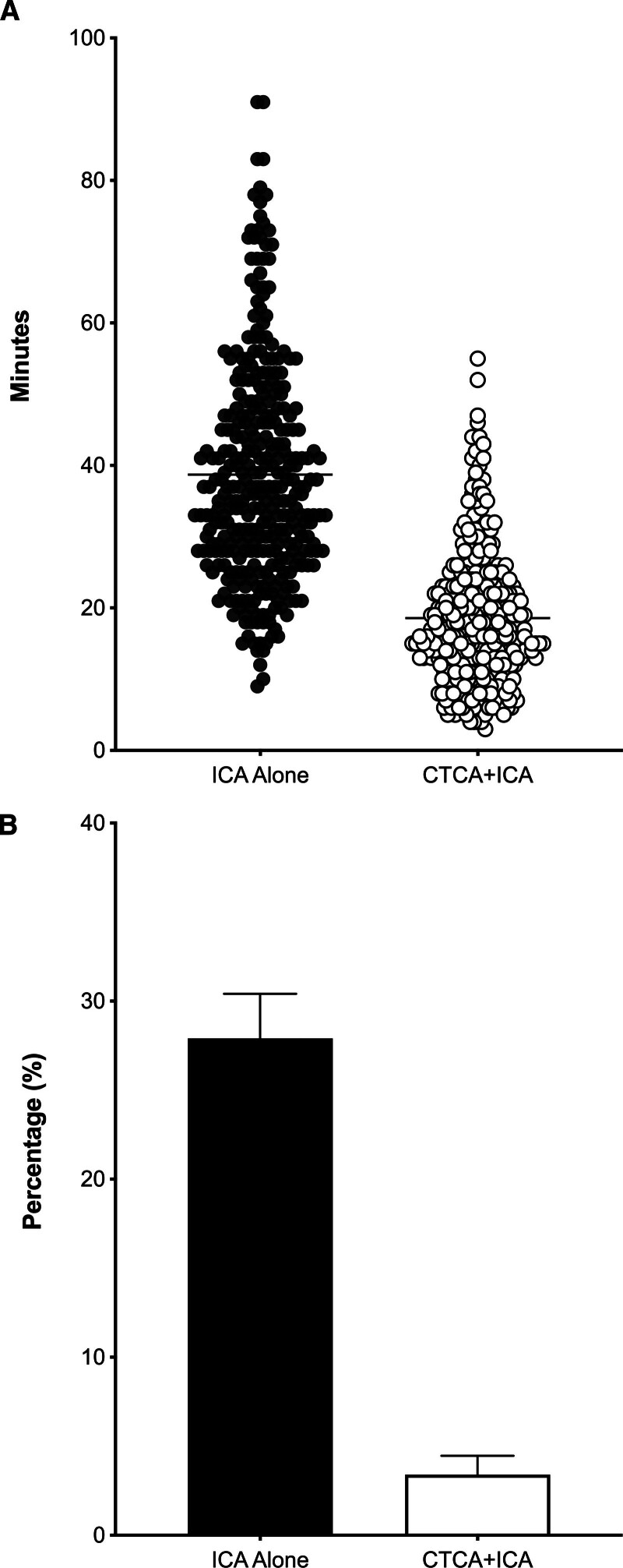
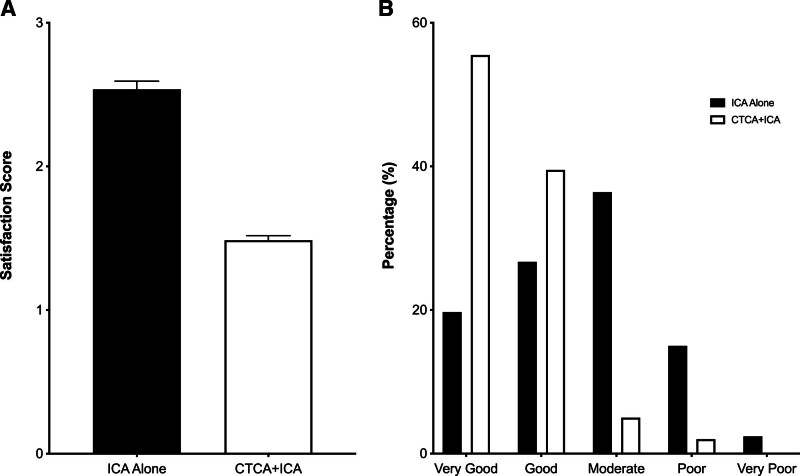
This study was a single-center, open-label randomized controlled trial assessing the benefit of adjunctive CTCA in patients with previous coronary artery bypass grafting referred for ICA. Patients were randomized 1:1 to undergo CTCA before ICA or ICA alone. The co-primary end points were procedural duration of the ICA (defined as the interval between local anesthesia administration for obtaining vascular access and removal of the last catheter), patient satisfaction after ICA using a validated questionnaire, and the incidence of contrast-induced nephropathy. Linear regression was used for procedural duration and patient satisfaction score; contrast-induced nephropathy was analyzed using logistic regression. We applied the Bonferroni correction, with <0.017 considered significant and 98.33% CIs presented. Secondary end points included incidence of procedural complications and 1-year major adverse cardiac events.
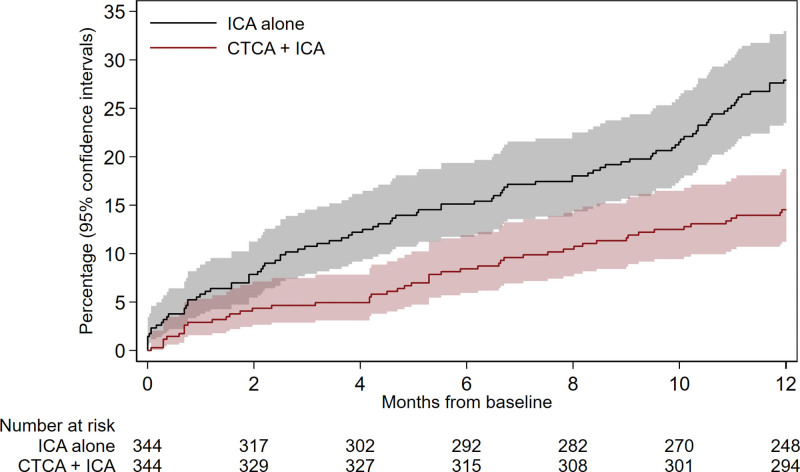
Over 3 years, 688 patients were randomized with a median follow-up of 1.0 years. The mean age was 69.8±10.4 years, 108 (15.7%) were women, 402 (58.4%) were White, and there was a high burden of comorbidity (85.3% hypertension and 53.8% diabetes). The median time from coronary artery bypass grafting to angiography was 12.0 years, and there were a median of 3 (interquartile range, 2 to 3) grafts per participant. Procedure duration of the ICA was significantly shorter in the CTCA+ICA group (CTCA+ICA, 18.6±9.5 minutes versus ICA alone, 39.5±16.9 minutes [98.33% CI, -23.5 to -18.4]; <0.001), alongside improved mean ICA satisfaction scores (1=very good to 5=very poor; -1.1 difference [98.33% CI, -1.2 to -0.9]; <0.001), and reduced incidence of contrast-induced nephropathy (3.4% versus 27.9%; odds ratio, 0.09 [98.33% CI, 0.04-0.2]; <0.001). Procedural complications (2.3% versus 10.8%; odds ratio, 0.2 [95% CI, 0.1-0.4]; <0.001) and 1-year major adverse cardiac events (16.0% versus 29.4%; hazard ratio, 0.4 [95% CI, 0.3-0.6]; <0.001) were also lower in the CTCA+ICA group.
For patients with previous coronary artery bypass grafting, CTCA before ICA leads to reductions in procedure time and contrast-induced nephropathy, with improved patient satisfaction. CTCA before ICA should be considered in this group of patients.
URL: https://www.
gov; Unique identifier: NCT03736018.
既往行冠状动脉旁路移植术的患者常需行有创性冠状动脉造影(ICA)。然而,对于这些患者,该操作技术上更具挑战性,且并发症风险更高。观察性研究表明,计算机断层扫描冠状动脉造影(CTCA)可能有助于该人群的 ICA,但尚未在随机对照试验中得到验证。
这是一项单中心、开放标签的随机对照试验,评估了 CTCA 对既往行冠状动脉旁路移植术并接受 ICA 患者的辅助作用。患者以 1:1 的比例随机分为 CTCA 联合 ICA 组或单纯 ICA 组。主要复合终点为 ICA 的操作时间(定义为局部麻醉用于获得血管通路至最后一根导管取出的时间间隔)、使用经过验证的问卷评估的 ICA 后患者满意度,以及对比剂肾病的发生率。线性回归用于分析操作时间和患者满意度评分;对比剂肾病采用逻辑回归进行分析。我们应用了 Bonferroni 校正,<0.017 认为有统计学意义,且给出 98.33%的置信区间。次要终点包括操作并发症发生率和 1 年主要不良心脏事件。
在 3 年内对 688 例患者进行了随机分组,中位随访时间为 1.0 年。患者的平均年龄为 69.8±10.4 岁,108 例(15.7%)为女性,402 例(58.4%)为白人,且合并症负担较高(85.3%为高血压,53.8%为糖尿病)。从冠状动脉旁路移植术到造影的中位时间为 12.0 年,每位患者平均有 3 个(四分位间距 2-3)桥血管。CTCA+ICA 组的 ICA 操作时间明显缩短(CTCA+ICA 组为 18.6±9.5 分钟,单纯 ICA 组为 39.5±16.9 分钟[98.33%置信区间,-23.5 至-18.4];<0.001),同时 ICA 满意度评分均值更高(1 分为非常好至 5 分为非常差;差值为-1.1[98.33%置信区间,-1.2 至-0.9];<0.001),且对比剂肾病的发生率更低(3.4%比 27.9%;比值比,0.09[98.33%置信区间,0.04-0.2];<0.001)。操作并发症(2.3%比 10.8%;比值比,0.2[95%置信区间,0.1-0.4];<0.001)和 1 年主要不良心脏事件(16.0%比 29.4%;风险比,0.4[95%置信区间,0.3-0.6];<0.001)在 CTCA+ICA 组也较低。
对于既往行冠状动脉旁路移植术的患者,在 ICA 前进行 CTCA 可减少操作时间和对比剂肾病,同时提高患者满意度。对于该类患者,应考虑在 ICA 前进行 CTCA。
网址:https://www.
gov;唯一标识符:NCT03736018。