Centro de Innovación en Salud ANCORA UC, Facultad de Medicina, Pontificia Universidad Católica de Chile, Santiago, Chile.
Health Technology Assessment Unit, Center of Clinical Research, Pontificia Universidad Católica de Chile, Santiago, Chile.
BMC Health Serv Res. 2023 Sep 29;23(1):1041. doi: 10.1186/s12913-023-09970-y.
Multimorbidity and patient-centered care approaches are growing challenges for health systems and patients. The cost of multimorbidity patients and the transition to a new care strategy is still sightly explored. In Chile, more than 70% of the adult population suffer from multimorbidity, opening an opportunity to implement a Multimorbidity patient-centered care model. The objective of this study was to perform an economic evaluation of the model from the public health system perspective.The methodology used a cost-consequence evaluation comparing seven exposed with seven unexposed primary care centers, and their reference hospitals. It followed three steps. First, we performed a Time-Driven Activity-Based Costing with routinely collected data routinely collected. Second, we run a comparative analysis through a propensity score matching and an estimation of the attributable costs to health services utilization at primary, secondary and tertiary care and health outcomes. Third, we estimated implementation and transaction costs.Results showed savings in aggregate costs of the total population (-0.12 (0.03) p < 0.01) during the period under evaluation. Costs in primary care showed a significant increase, whereas tertiary care showed significant savings. Health outcomes were associated with higher survival in patients under the new care model (HR 0.70 (0.05) p < 0.01). Implementation and transaction costs increased as the number of pilot intervention centers increased, and they represented 0,07% of the total annual budget of the Servicio de Salud Metropolitano Sur Oriente. After three years of piloting, the implementation and transaction cost for the total period was USD 1,838,767 and 393,775, respectively.The study's findings confirm the purpose of the new model to place primary health care at the center of care for people with non-communicable chronic diseases. Thus, it is necessary to consider implementation and transaction costs to introduce a broad health system multimorbidity approach. The health system should assume some of them permanently to guarantee sustainability and facilitate scale-up.
多病共存和以患者为中心的护理方法是卫生系统和患者面临的日益严峻的挑战。多病共存患者的成本以及向新护理策略的转变仍在探索之中。在智利,超过 70%的成年人口患有多病共存,这为实施多病共存患者为中心的护理模式提供了机会。本研究旨在从公共卫生系统的角度对该模式进行经济评估。
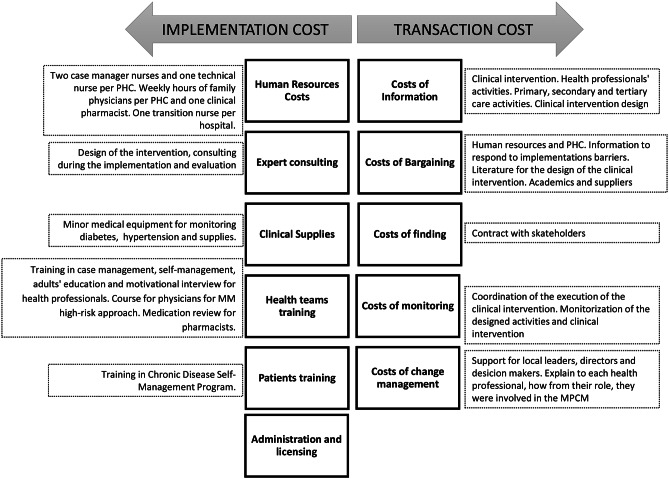
该方法采用成本-后果评估,比较了 7 个暴露组和 7 个未暴露组的初级保健中心及其参考医院。它分为三个步骤。首先,我们使用基于时间的活动成本核算方法,使用常规收集的数据进行核算。其次,通过倾向评分匹配和对初级、二级和三级医疗保健服务利用和健康结果的归因成本进行比较分析。最后,我们估计了实施和交易成本。
结果表明,在评估期间,总人口的总费用(-0.12(0.03)p<0.01)有所节省。初级保健的成本显著增加,而三级保健的成本显著节省。健康结果与新护理模式下患者的生存率提高有关(HR 0.70(0.05)p<0.01)。随着试点干预中心数量的增加,实施和交易成本增加,占南方大都会卫生局总年度预算的 0.07%。经过三年的试点,整个试点期间的实施和交易成本分别为 1838767 美元和 393775 美元。
研究结果证实了新模型的目的,即将初级卫生保健置于非传染性慢性病患者护理的中心位置。因此,有必要考虑实施和交易成本,以引入广泛的卫生系统多病共存方法。卫生系统应永久性地承担其中的一些成本,以确保可持续性并促进扩大规模。