NIHR Policy Research Unit in Maternal and Neonatal Health and Care, National Perinatal Epidemiology Unit, Nuffield Department of Population Health, University of Oxford, Oxford, United Kingdom.
Reproduction and Perinatal Centre, Faculty of Medicine and Health, University of Sydney, Sydney, Australia.
PLoS One. 2023 Oct 5;18(10):e0291795. doi: 10.1371/journal.pone.0291795. eCollection 2023.
To estimate the incidence of, and investigate risk factors for, postpartum haemorrhage (PPH) requiring transfer to obstetric care following birth in midwifery units (MU) in the UK; to describe outcomes for women who experience PPH requiring transfer to obstetric care.
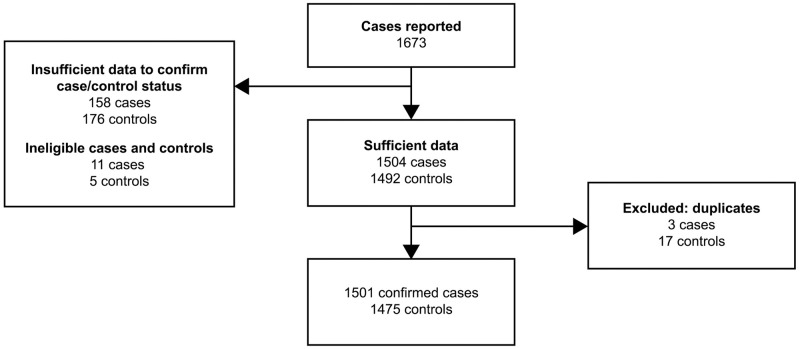
We conducted a national population-based case-control study in all MUs in the UK using the UK Midwifery Study System (UKMidSS). Between September 2019 and February 2020, 1501 women with PPH requiring transfer to obstetric care following birth in an MU, and 1475 control women were identified. We used multivariable logistic regression, generating adjusted odds ratios (aORs) and 95% confidence intervals (CIs) to investigate risk factors for PPH requiring transfer to obstetric care.
The incidence of PPH requiring transfer to obstetric care following birth in an MU was 3.7% (95% CI 3.6%-3.9%). Factors independently associated with PPH requiring transfer to obstetric care were smoking during pregnancy (aOR = 0.73; 95% CI 0.56-0.94), nulliparity (aOR = 1.96; 95% CI 1.66-2.30), previous PPH (aOR = 2.67; 95% CI 1.67-4.25), complications in a previous pregnancy other than PPH (aOR = 2.40; 95% CI 1.25-4.60), gestational age ≥41 weeks (aOR = 1.36; 95% CI 1.10-1.69), instrumental birth (aOR = 2.69; 95% CI 1.53-4.72), third stage of labour ≥60 minutes (aOR = 5.56; 95% CI 3.93-7.88), perineal trauma (aOR = 4.67; 95% CI 3.16-6.90), and birthweight 3500-3999g (aOR = 1.71; 95% CI 1.42-2.07) or ≥4000g (aOR = 2.31; 95% CI 1.78-3.00). One in ten (10.6%) cases received a blood transfusion and one in five (21.0%) were admitted to higher level care.
The risk factors identified in this study align with those identified in previous research and with current guidelines for women planning birth in an MU in the UK. Maternal outcomes after PPH were broadly reassuring and indicative of appropriate management. NHS organisations should ensure that robust guidelines are in place to support management of PPH in MUs.
估计在英国助产单位(MU)分娩后因产后出血(PPH)需要转至产科护理的发生率,并探讨其危险因素;描述因 PPH 需要转至产科护理的妇女的结局。
我们在英国所有 MU 中使用英国助产士研究系统(UKMidSS)开展了一项全国性基于人群的病例对照研究。在 2019 年 9 月至 2020 年 2 月期间,我们在 MU 分娩后因 PPH 需要转至产科护理的 1501 名妇女和 1475 名对照妇女中确定了病例和对照。我们使用多变量逻辑回归,生成调整后的优势比(aOR)和 95%置信区间(CI)来探讨需要转至产科护理的 PPH 的危险因素。
MU 分娩后因 PPH 需要转至产科护理的发生率为 3.7%(95%CI 3.6%-3.9%)。与需要转至产科护理的 PPH 独立相关的因素包括孕期吸烟(aOR=0.73;95%CI 0.56-0.94)、初产(aOR=1.96;95%CI 1.66-2.30)、既往 PPH(aOR=2.67;95%CI 1.67-4.25)、除 PPH 以外的既往妊娠并发症(aOR=2.40;95%CI 1.25-4.60)、胎龄≥41 周(aOR=1.36;95%CI 1.10-1.69)、器械分娩(aOR=2.69;95%CI 1.53-4.72)、第三产程≥60 分钟(aOR=5.56;95%CI 3.93-7.88)、会阴创伤(aOR=4.67;95%CI 3.16-6.90)、出生体重 3500-3999g(aOR=1.71;95%CI 1.42-2.07)或≥4000g(aOR=2.31;95%CI 1.78-3.00)。十分之一(10.6%)的病例接受了输血,五分之一(21.0%)的病例被收治到更高一级的护理病房。
本研究确定的危险因素与既往研究和英国 MU 分娩计划的当前指南中确定的危险因素一致。PPH 后的产妇结局普遍令人安心,表明管理得当。NHS 组织应确保制定健全的指南,以支持 MU 中 PPH 的管理。