Panagiota Victoria, Kerschbaum Johanna Franziska, Penack Olaf, Stein Catarina M, Arends Christopher M, Koenecke Christian, Strzelecka Paulina M, Kloos Arnold, Wiegand Laura, Lasch Alina, Altwasser Robert, Halik Adriane, Gabdoulline Razif, Thomson Julia, Weibl Konstantin, Franke Georg-Nikolaus, Berger Carolina, Hasenkamp Justin, Ayuk Francis, Na Il-Kang, Beutel Gernot, Keller Ulrich, Bullinger Lars, Wulf Gerald Georg, Kröger Nicolaus, Vucinic Vladan, Heuser Michael, Damm Frederik
Department of Hematology, Hemostasis, Oncology and Stem Cell Transplantation, Hannover Medical School, Hannover, Germany.
Department of Hematology, Oncology, and Cancer Immunology, Charité - Universitätsmedizin Berlin, corporate member of Freie Universität Berlin, Humboldt-Universität zu Berlin, Germany.
Hemasphere. 2023 Oct 3;7(10):e957. doi: 10.1097/HS9.0000000000000957. eCollection 2023 Oct.
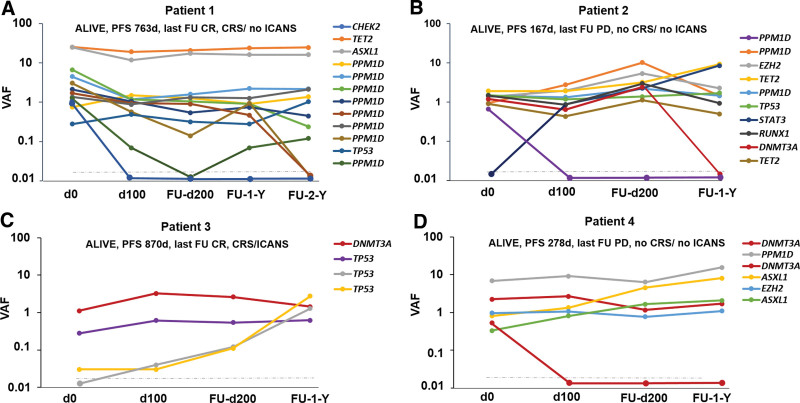
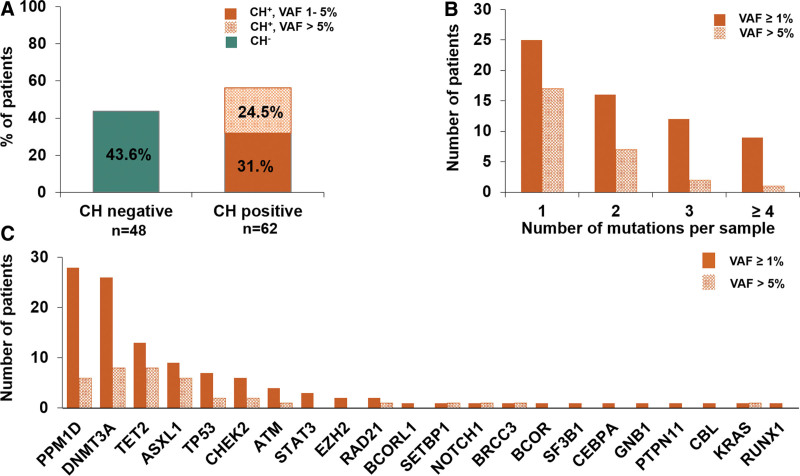
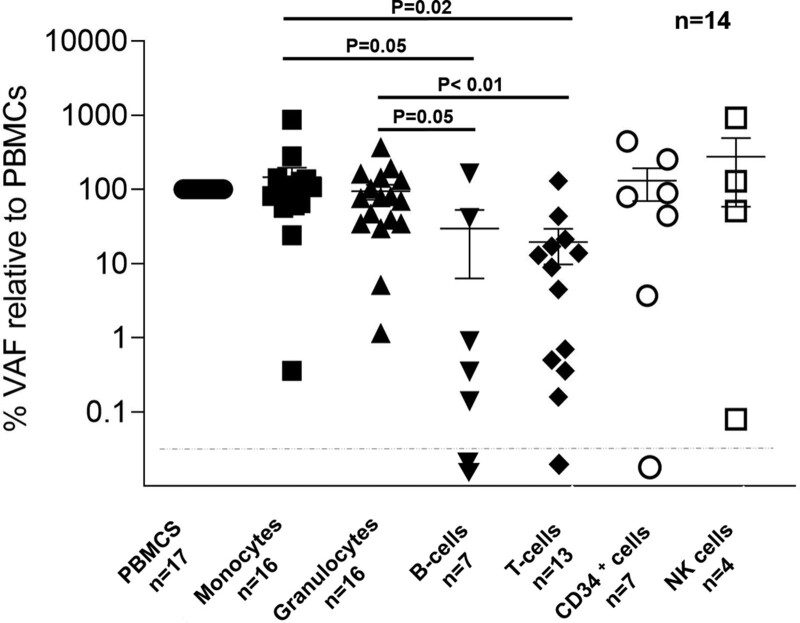
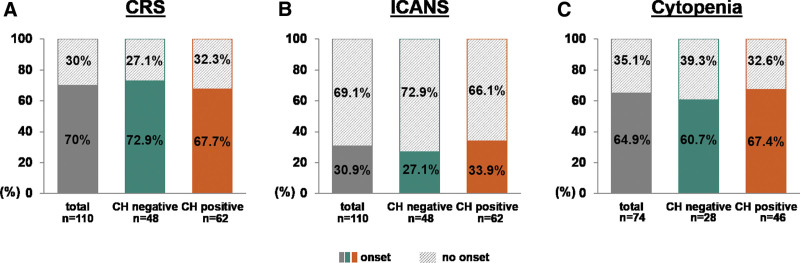
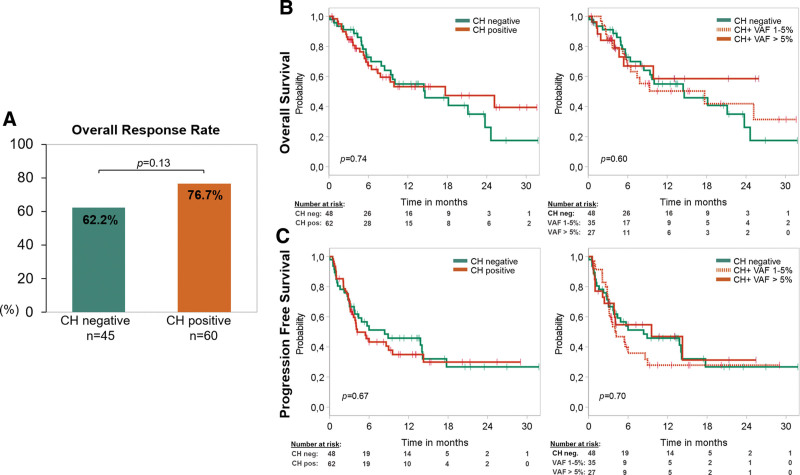
Recent evidence revealed important interactions between clonal hematopoiesis (CH) and cellular therapies established for the treatment of hematologic malignancies. The impact of CH on safety, efficacy, and outcome of chimeric antigen receptor (CAR) T-cell therapy is currently under investigation. We analyzed 110 patients with relapsed/refractory B-cell non-Hodgkin lymphoma (n = 105) or acute lymphoblastic leukemia (ALL) (n = 5), treated with Axicabtagene-Ciloleucel (39%), Tisagenlecleucel (51%), or Brexucabtagene autoleucel (10%). Using error-corrected targeted sequencing, a high CH prevalence of 56.4% (variant allele frequency [VAF] ≥1%) at the time of CAR T-cell infusion was detected. The most frequently mutated gene was followed by , , , and . Variant allele frequencies were significantly lower in B and T cells compared with monocytes and granulocytes. CH did not increase the risk of CAR T-related toxicities. The incidences of cytokine release syndrome and immune effector-cell-associated neurotoxicity syndrome were similar between CH and CH patients, regardless of clone size, age, or CAR T product. Prolonged cytopenias were not associated with CH. Best overall response rates (ORRs) were numerically but not significantly higher in CH patients (ORR 76.7% versus 62.2%; = 0.13). Furthermore, CH status did not predict progression-free survival or overall survival. Lastly, sequential analysis showed a modest VAF increase of 1.3% and acquisition of novel mutations within 100 days postinfusion. CH was frequent in large B-cell lymphoma/ALL patients receiving CAR T-cells but did not affect toxicity nor treatment response or outcome.
近期证据显示,克隆性造血(CH)与用于治疗血液系统恶性肿瘤的细胞疗法之间存在重要相互作用。目前正在研究CH对嵌合抗原受体(CAR)T细胞疗法的安全性、疗效和结果的影响。我们分析了110例复发/难治性B细胞非霍奇金淋巴瘤(n = 105)或急性淋巴细胞白血病(ALL)(n = 5)患者,这些患者接受了阿基仑赛(39%)、替雷利珠单抗(51%)或布雷西尤单抗(10%)治疗。采用纠错靶向测序法,在CAR T细胞输注时检测到CH的高患病率为56.4%(变异等位基因频率[VAF]≥1%)。最常发生突变的基因依次为 , , , 和 。与单核细胞和粒细胞相比,B细胞和T细胞中的变异等位基因频率显著更低。CH并未增加CAR T相关毒性的风险。无论克隆大小、年龄或CAR T产品如何,CH患者与非CH患者之间的细胞因子释放综合征和免疫效应细胞相关神经毒性综合征的发生率相似。血细胞减少持续时间延长与CH无关。CH患者的最佳总体缓解率(ORR)在数值上较高,但无显著差异(ORR 76.7%对62.2%; = 0.13)。此外,CH状态无法预测无进展生存期或总生存期。最后,序贯分析显示输注后100天内变异等位基因频率适度增加1.3%并出现新的突变。接受CAR T细胞治疗的大B细胞淋巴瘤/ALL患者中CH很常见,但不影响毒性、治疗反应或结果。