Baek Jang-Hyun, Heo Ji Hoe, Nam Hyo Suk, Kim Byung Moon, Kim Dong Joon, Kim Young Dae
Department of Neurology, Kangbuk Samsung Hospital, Sungkyunkwan University School of Medicine, Seoul 03181, Republic of Korea.
Department of Neurology, Severance Stroke Center, Severance Hospital, Yonsei University College of Medicine, Seoul 03722, Republic of Korea.
J Clin Med. 2023 Sep 29;12(19):6289. doi: 10.3390/jcm12196289.
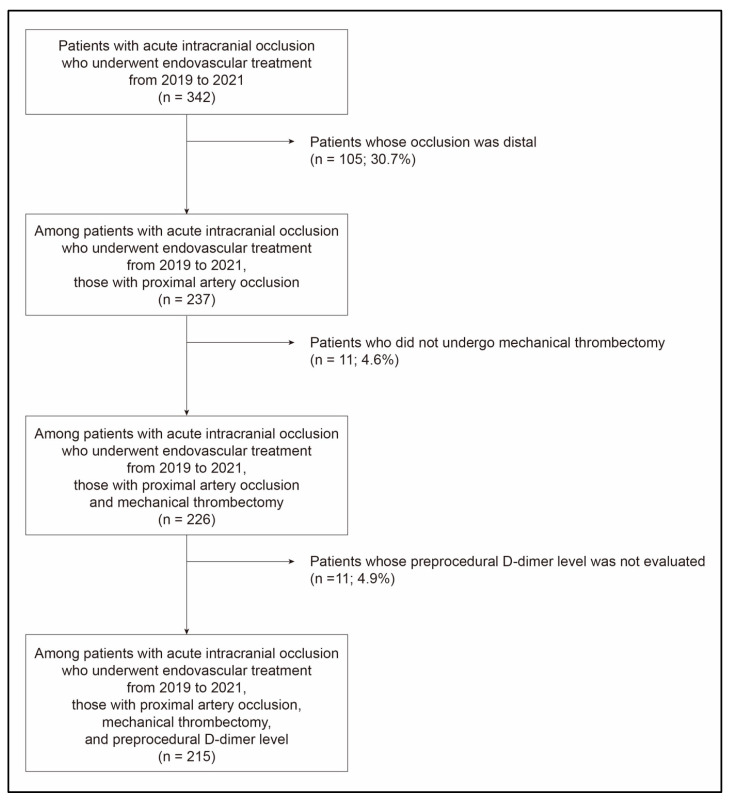
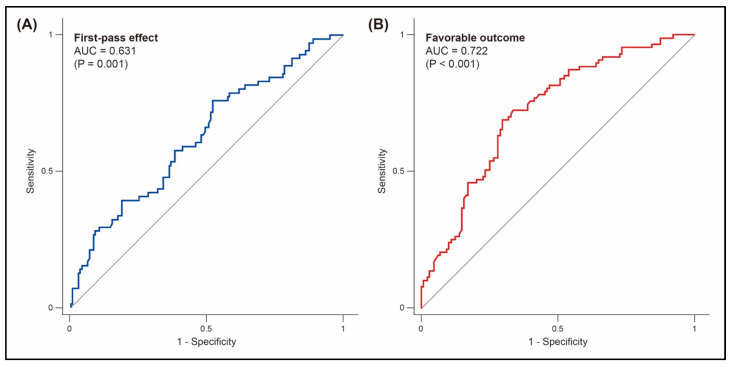
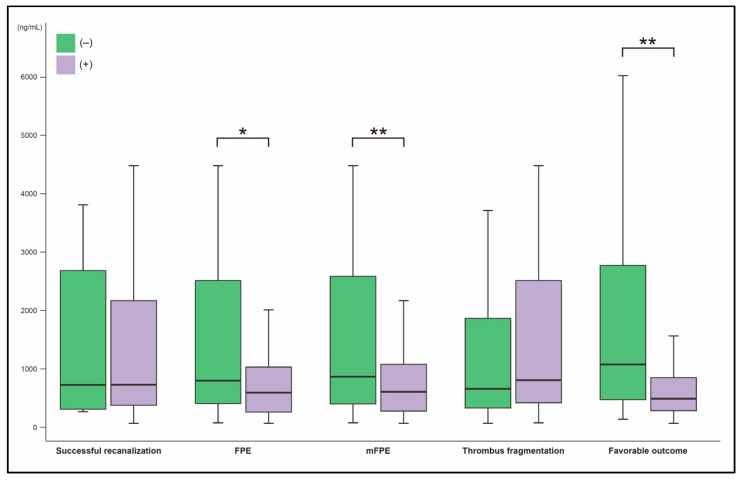
We aimed to evaluate the association between preprocedural D-dimer levels and endovascular and clinical outcomes. We retrospectively reviewed patients with acute intracranial large-vessel occlusion who underwent mechanical thrombectomy. Plasma D-dimer levels were measured immediately before the endovascular procedure. Endovascular outcomes included successful recanalization, first-pass recanalization (first-pass effect (FPE) and modified FPE (mFPE)), thrombus fragmentation, and the number of passes of the thrombectomy device. Clinical outcomes were assessed at 3 months using the modified Rankin Scale. A total of 215 patients were included. Preprocedural D-dimer levels were lower in patients with FPE (606.0 ng/mL [interquartile range, 268.0-1062.0]) than in those without (879.0 ng/mL [437.0-2748.0]; = 0.002). Preprocedural D-dimer level was the only factor affecting FPE (odds ratio, 0.92 [95% confidence interval, 0.85-0.98] per 500 ng/mL; = 0.022). D-dimer levels did not differ significantly based on successful recanalization and thrombus fragmentation. The number of passes of the thrombectomy device was higher ( = 0.002 for trend) and the puncture-to-recanalization time was longer ( = 0.044 for trend) as the D-dimer levels increased. Patients with favorable outcome had significantly lower D-dimer levels (495.0 ng/mL [290.0-856.0]) than those without (1189.0 ng/mL [526.0-3208.0]; < 0.001). Preprocedural D-dimer level was an independent factor for favorable outcome (adjusted odds ratio, 0.88 [0.81-0.97] per 500 ng/mL; = 0.008). In conclusion, higher preprocedural D-dimer levels were significantly associated with poor endovascular and unfavorable functional outcomes.
我们旨在评估术前D-二聚体水平与血管内治疗结局及临床结局之间的关联。我们回顾性分析了接受机械取栓术的急性颅内大血管闭塞患者。在血管内治疗前即刻测量血浆D-二聚体水平。血管内治疗结局包括成功再通、首次通过再通(首次通过效应(FPE)和改良首次通过效应(mFPE))、血栓破碎以及取栓装置的通过次数。使用改良Rankin量表在3个月时评估临床结局。共纳入215例患者。FPE患者的术前D-二聚体水平(606.0 ng/mL[四分位间距,268.0 - 1062.0])低于无FPE患者(879.0 ng/mL[437.0 - 2748.0];P = 0.002)。术前D-二聚体水平是影响FPE的唯一因素(比值比,0.92[95%置信区间,0.85 - 0.98]每500 ng/mL;P = 0.022)。基于成功再通和血栓破碎情况,D-二聚体水平无显著差异。随着D-二聚体水平升高,取栓装置的通过次数增加(趋势P = 0.002),穿刺至再通时间延长(趋势P = 0.044)。预后良好的患者D-二聚体水平(495.0 ng/mL[290.0 - 856.0])显著低于预后不良患者(1189.0 ng/mL[526.0 - 3208.0];P < 0.001)。术前D-二聚体水平是预后良好的独立因素(校正比值比,0.88[0.81 - 0.97]每500 ng/mL;P = 0.008)。总之,术前较高的D-二聚体水平与不良的血管内治疗结局和不利的功能结局显著相关。