International Renal Research Institute of Vicenza Institute of Vicenza, San Bortolo Hospital, Vicenza, Italy.
Department of Anesthesiology and Intensive Care, San Bortolo Hospital, Vicenza, Italy.
Sci Rep. 2023 Oct 16;13(1):17600. doi: 10.1038/s41598-023-44850-9.
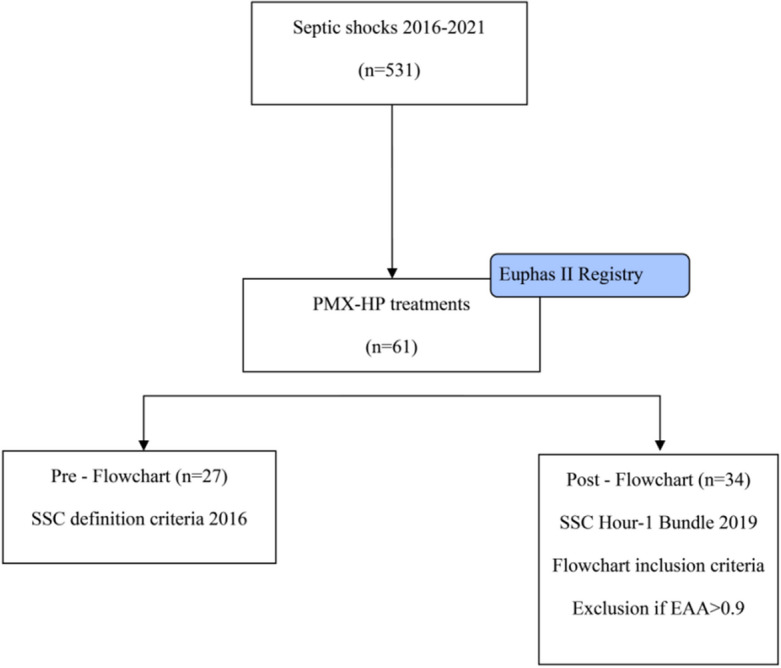
Although the precise clinical indication for initiation of PMX-HA is widely debated in the literature, a proper patient selection and timing of treatment delivery might play a critical role in the clinical course of a specific subphenotype of septic shock (endotoxic shock). In light of this view, since 2019, we have introduced in our clinical practice a diagnostic-therapeutic flowchart to select patients that can benefit the most from the treatment proposed. In addition, we reported in this study our experience of PMX-HA in a cohort of critically ill patients admitted to our intensive care unit (ICU). We analyzed a single centre, retrospective, observational web-based database (extracted from the EUPHAS2 registry) of critically ill patients admitted to the ICU between January 2016 and May 2021 who were affected by endotoxic shock. Patients were divided according to the diagnostic-therapeutic flowchart in two groups: Pre-Flowchart (Pre-F) and Post-Flowchart (Post-F). From January 2016 to May 2021, 61 patients were treated with PMX-HA out of 531 patients diagnosed with septic shock and of these, fifty patients (82%) developed AKI during their ICU stay. The most common source of infection was secondary peritonitis (36%), followed by community-acquired pneumonia (29%). Fifty-five (90%) out of 61 patients received a second PMX-HA treatment, with a statistically significant difference between the two groups (78% of the Pre-F vs. 100% of the Post-F group, p = 0.005). In both groups, between T0 and T120, the Endotoxin Activity Assay (EAA) decreased, while the SOFA score, mean arterial pressure (MAP), and Vasoactive Inotropic Score (VIS) improved with no statistically significant difference. Furthermore, when performing a propensity score matching analysis to compare mortality between the two groups, statistically significant lower ICU and 90-day mortalities were observed in the Post-F group [p = 0.016]. Although in this experienced centre data registry, PMX-HA was associated with organ function recovery, hemodynamic improvement, and current EAA level reduction in critically ill patients with endotoxic shock. Following propensity score-matched analysis, ICU mortality and 90-day mortalities were lower in the diagnostic-therapeutic flowchart group when considering two temporal groups based on strict patient selection criteria and timing to achieve PMX. Further Randomised Control Trials focused on centre selection, adequate training and a flowchart of action when assessing extracorporeal blood purification use should be performed.
虽然 PMX-HA 启动的确切临床指征在文献中存在广泛争议,但适当的患者选择和治疗时机的把握可能对特定类型感染性休克(内毒素性休克)的临床病程起着关键作用。基于这一观点,自 2019 年以来,我们在临床实践中引入了一种诊断-治疗流程图,以选择最能从所提议的治疗中受益的患者。此外,我们在这项研究中报告了我们在重症监护病房(ICU)收治的一组危重症患者中使用 PMX-HA 的经验。我们分析了 2016 年 1 月至 2021 年 5 月期间在 ICU 收治的受内毒素性休克影响的危重症患者的单中心、回顾性、基于网络的数据库(从 EUPHAS2 登记处提取),这些患者均接受了 PMX-HA 治疗。患者根据诊断-治疗流程图分为两组:流程图前(Pre-F)和流程图后(Post-F)。2016 年 1 月至 2021 年 5 月,531 例确诊为感染性休克的患者中有 61 例接受了 PMX-HA 治疗,其中 50 例(82%)在 ICU 期间发生 AKI。最常见的感染源是继发性腹膜炎(36%),其次是社区获得性肺炎(29%)。55 例(90%)患者接受了第二次 PMX-HA 治疗,两组间差异有统计学意义(Pre-F 组为 78%,Post-F 组为 100%,p=0.005)。两组患者在 T0 至 T120 期间,内毒素活性检测(EAA)降低,而 SOFA 评分、平均动脉压(MAP)和血管活性药物评分(VIS)改善,差异无统计学意义。此外,在进行倾向评分匹配分析比较两组死亡率时,Post-F 组 ICU 死亡率和 90 天死亡率均显著降低(p=0.016)。虽然在这个经验丰富的中心数据登记中,PMX-HA 与器官功能恢复、血流动力学改善和当前内毒素水平降低有关,但其对感染性休克伴内毒素血症的危重症患者的影响仍需进一步研究。在基于严格的患者选择标准和实现 PMX 的时间进行倾向性评分匹配分析后,流程图组的 ICU 死亡率和 90 天死亡率较低。考虑到基于中心选择、充分培训和评估体外血液净化使用流程图的两个时间组,应进行更多的随机对照试验。