School of Nursing, University of Ottawa, 200 Lees Avenue, Ottawa, ON, K1N 6N5, Canada.
Clinical Epidemiology Program, Ottawa Hospital Research Institute, 501 Smyth Road, Ottawa, ON, K1H 8L6, Canada.
BMC Pregnancy Childbirth. 2023 Oct 17;23(1):735. doi: 10.1186/s12884-023-06042-1.
Moving evidence into practice is complex, and pregnant and birthing people and their infants do not always receive care that aligns with the best available evidence. Implementation science can inform how to effectively move evidence into practice. While there are a growing number of examples of implementation science being studied in maternal-newborn care settings, it remains unknown how real-world teams of healthcare providers and leaders approach the overall implementation process when making practice changes. The purpose of this study was to describe maternal-newborn hospital teams' approaches to implementing practice changes. We aimed to identify what implementation steps teams take (or not) and identify strengths and potential areas for improvement based on best practices in implementation science.
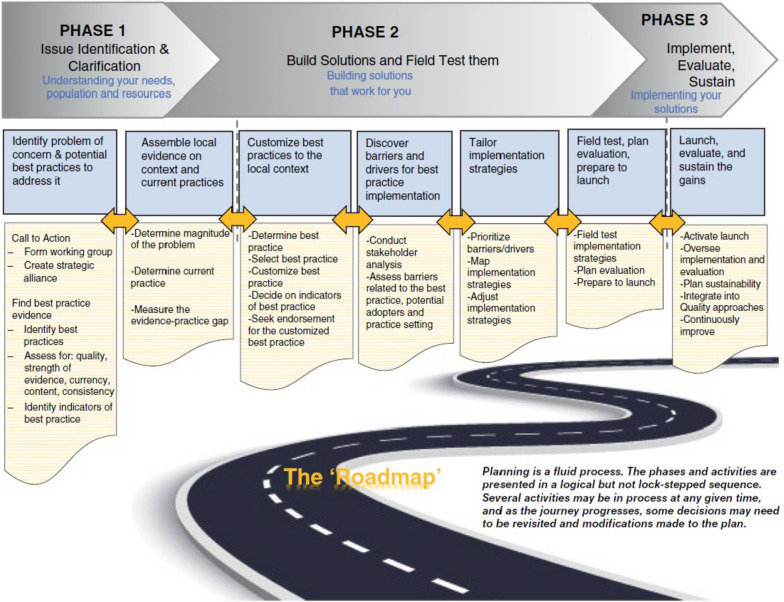
We conducted a supplementary qualitative secondary analysis of 22 interviews completed in 2014-2015 with maternal-newborn nursing leaders in Ontario, Canada. We used directed content analysis to code the data to seven steps in an implementation framework (Implementation Roadmap): identify the problem and potential best practice; assemble local evidence; select and customize best practice; discover barriers and drivers; tailor implementation strategies; field-test, plan evaluation, prepare to launch; launch, evaluate, and sustain. Frequency counts are presented for each step.
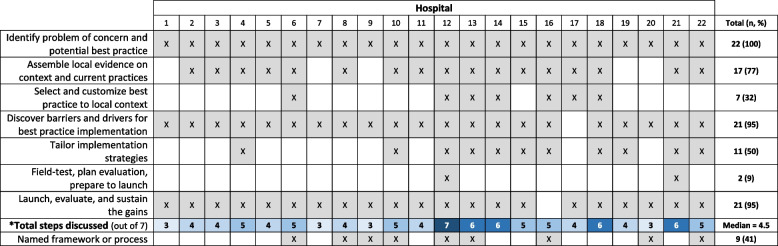
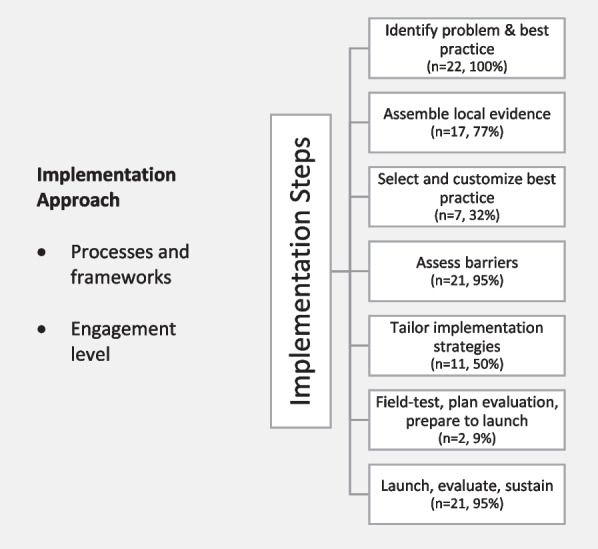
Participants reported completing a median of 4.5 of 7 Implementation Roadmap steps (range = 3-7), with the most common being identifying a practice problem. Other steps were described less frequently (e.g., selecting and adapting evidence, field-testing, outcome evaluation) or discussed frequently but not optimally (e.g., barriers assessment). Participants provided examples of how they engaged point-of-care staff throughout the implementation process, but provided fewer examples of engaging pregnant and birthing people and their families. Some participants stated they used a formal framework or process to guide their implementation process, with the most common being quality improvement approaches and tools.
We identified variability across the 22 hospitals in the implementation steps taken. While we observed many strengths, we also identified areas where further support may be needed. Future work is needed to create opportunities and resources to support maternal-newborn healthcare providers and leaders to apply principles and tools from implementation science to their practice change initiatives.
将证据付诸实践是复杂的,孕妇和分娩的妇女及其婴儿并不总是接受符合最佳现有证据的护理。实施科学可以为如何有效地将证据付诸实践提供信息。虽然在孕产妇护理环境中研究实施科学的例子越来越多,但仍不清楚医疗保健提供者和领导者的实际团队在进行实践变革时如何整体实施过程。本研究的目的是描述孕产妇医院团队实施实践变革的方法。我们旨在确定团队采取了哪些(或没有)实施步骤,并根据实施科学的最佳实践确定优势和潜在改进领域。
我们对 2014-2015 年在加拿大安大略省进行的 22 次与孕产妇护理领导者的访谈进行了补充定性二次分析。我们使用定向内容分析对数据进行编码,分为实施框架(实施路线图)的七个步骤:确定问题和潜在最佳实践;收集当地证据;选择和定制最佳实践;发现障碍和驱动力;调整实施策略;现场测试、计划评估、准备启动;启动、评估和维持。每个步骤都呈现了频率计数。
参与者报告完成了实施路线图的 7 个步骤中的中位数为 4.5 个(范围为 3-7),最常见的是确定实践问题。其他步骤的描述频率较低(例如,选择和调整证据、现场测试、结果评估)或讨论频率较高但不理想(例如,障碍评估)。参与者提供了他们在实施过程中如何让护理人员参与的例子,但提供了较少让孕妇和分娩的妇女及其家属参与的例子。一些参与者表示他们使用了正式的框架或流程来指导他们的实施过程,最常见的是质量改进方法和工具。
我们在 22 家医院的实施步骤中发现了差异。虽然我们观察到了许多优势,但我们也确定了需要进一步支持的领域。未来需要开展工作,创造机会和资源,支持孕产妇保健提供者和领导者将实施科学的原则和工具应用于他们的实践变革计划。