Pablo Arturo Suarez Hospital, Intensive Care Unit, Clinical Research Center, Quito, Ecuador.
Faculty of Medical Sciences, Central University of Ecuador, Quito, Ecuador.
BMC Pulm Med. 2023 Oct 18;23(1):393. doi: 10.1186/s12890-023-02691-2.
In 2020, Ecuador had one of the highest death rates because of COVID-19. The role of clinical and biomolecular markers in COVID disease prognosis, is still not well supported by available data. In order for these markers to have practical application in clinical decision-making regarding patient treatment and prognosis, it is necessary to know an optimal cut-off point, taking into consideration ethnic differences and geographic conditions.
To determine the value of clinical and biomolecular markers, to predict mortality of patients with severe COVID-19 living at high altitude.
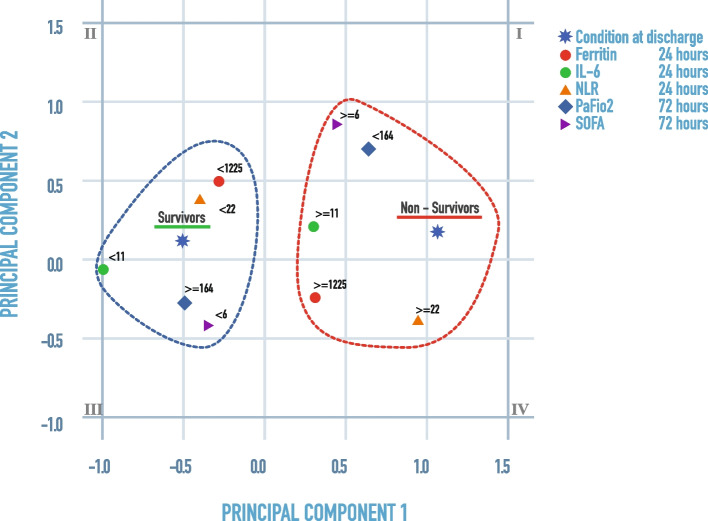
In this study, receiver operating characteristic (ROC) curves, area under the curve (AUC) of ROC, sensitivity, specificity and likelihood ratios were calculated to determine levels of clinical and biomolecular markers that best differentiate survivors versus non-survivors in severe COVID subjects that live at a high altitude setting.
Selected cut-off values for ferritin (≥ 1225 ng/dl, p = 0.026), IL-6 (≥ 11 pg/ml, p = 0.005) and NLR (≥ 22, p = 0.008) at 24 h, as well as PaFiO2 (≤ 164 mmHg, p = 0.015), NLR (≥ 16, p = p = 0.013) and SOFA (≥ 6, p = 0.031) at 72 h, appear to have good discriminating power to differentiate survivors versus non-survivors. Additionally, odds ratios for ferritin (OR = 3.38); IL-6 (OR = 17.07); PaFiO2 (OR = 4.61); NLR 24 h (OR = 4.95); NLR 72 h (OR = 4.46), and SOFA (OR = 3.77) indicate increased risk of mortality when cut-off points were taken into consideration.
We proposed a straightforward and understandable method to identify dichotomized levels of clinical and biomolecular markers that can discriminate between survivors and non-survivors patients with severe COVID-19 living at high altitudes.
2020 年,厄瓜多尔因 COVID-19 导致的死亡率居高不下。临床和生物标志物在 COVID 疾病预后中的作用,尚未得到现有数据的充分支持。为了使这些标志物在临床决策中对患者的治疗和预后具有实际应用价值,有必要考虑到种族差异和地理条件,确定一个最佳的截断点。
确定临床和生物标志物的价值,以预测生活在高海拔地区的重症 COVID-19 患者的死亡率。
本研究通过计算受试者工作特征(ROC)曲线、ROC 曲线下面积(AUC)、灵敏度、特异性和似然比,来确定在生活在高海拔地区的重症 COVID 患者中,能够最佳区分幸存者与非幸存者的临床和生物标志物的水平。
选择铁蛋白(≥1225ng/dl,p=0.026)、白细胞介素-6(≥11pg/ml,p=0.005)和 NLR(≥22,p=0.008)在 24 小时的截断值,以及 PaFiO2(≤164mmHg,p=0.015)、NLR(≥16,p=0.013)和 SOFA(≥6,p=0.031)在 72 小时的截断值,似乎具有良好的区分能力,可以区分幸存者与非幸存者。此外,铁蛋白(OR=3.38);白细胞介素-6(OR=17.07);PaFiO2(OR=4.61);NLR 24 小时(OR=4.95);NLR 72 小时(OR=4.46)和 SOFA(OR=3.77)的比值比表明,当考虑到截断值时,这些标志物的风险比增加,死亡风险更高。
我们提出了一种简单易懂的方法,用于识别可以区分生活在高海拔地区的重症 COVID-19 患者幸存者与非幸存者的临床和生物标志物的二分水平。