Metry Elisabeth L, Garrelfs Sander F, Deesker Lisa J, Acquaviva Cecile, D'Ambrosio Viola, Bacchetta Justine, Beck Bodo B, Cochat Pierre, Collard Laure, Hogan Julien, Ferraro Pietro Manuel, Franssen Casper F M, Harambat Jérôme, Hulton Sally-Anne, Lipkin Graham W, Mandrile Giorgia, Martin-Higueras Cristina, Mohebbi Nilufar, Moochhala Shabbir H, Neuhaus Thomas J, Prikhodina Larisa, Salido Eduardo, Topaloglu Rezan, Oosterveld Michiel J S, Groothoff Jaap W, Peters-Sengers Hessel
Department of Pediatric Nephrology, Emma Children's Hospital, Amsterdam UMC, University of Amsterdam, Amsterdam, The Netherlands.
Service de Biochimie et Biologie Moléculaire, UM Pathologies Héréditaires du Métabolisme et du Globule Rouge, Hospices Civils de Lyon, France.
Kidney Int Rep. 2023 Aug 4;8(10):2029-2042. doi: 10.1016/j.ekir.2023.07.025. eCollection 2023 Oct.
Primary hyperoxaluria type 1 (PH1) has a highly heterogeneous disease course. Apart from the c.508G>A (p.Gly170Arg) variant, which imparts a relatively favorable outcome, little is known about determinants of kidney failure. Identifying these is crucial for disease management, especially in this era of new therapies.
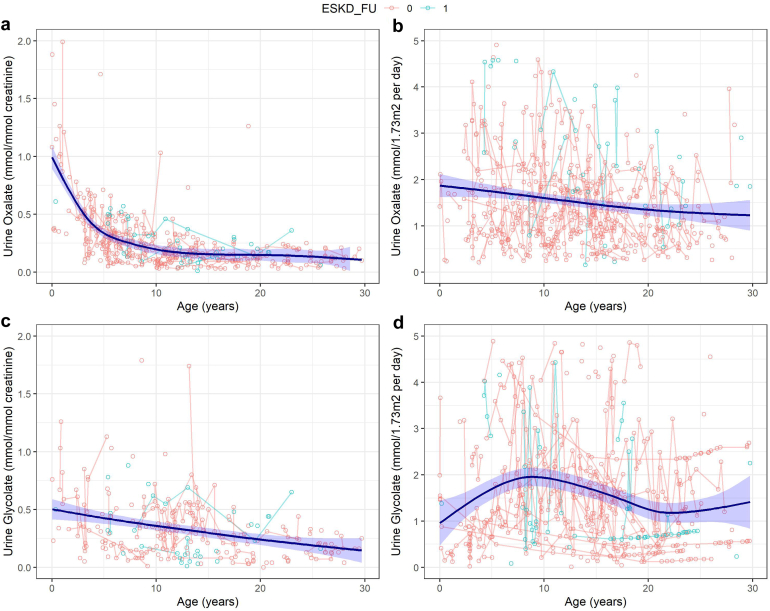
In this retrospective study of 932 patients with PH1 included in the OxalEurope registry, we analyzed genotype-phenotype correlations as well as the impact of nephrocalcinosis, urolithiasis, and urinary oxalate and glycolate excretion on the development of kidney failure, using survival and mixed model analyses.
The risk of developing kidney failure was the highest for 175 vitamin-B6 unresponsive ("null") homozygotes and lowest for 155 patients with c.508G>A and c.454T>A (p.Phe152Ile) variants, with a median age of onset of kidney failure of 7.8 and 31.8 years, respectively. Fifty patients with c.731T>C (p.Ile244Thr) homozygote variants had better kidney survival than null homozygotes ( = 0.003). Poor outcomes were found in patients with other potentially vitamin B6-responsive variants. Nephrocalcinosis increased the risk of kidney failure significantly (hazard ratio [HR] 3.17 [2.03-4.94], < 0.001). Urinary oxalate and glycolate measurements were available in 620 and 579 twenty-four-hour urine collections from 117 and 87 patients, respectively. Urinary oxalate excretion, unlike glycolate, was higher in patients who subsequently developed kidney failure ( = 0.034). However, the 41% intraindividual variation of urinary oxalate resulted in wide confidence intervals.
In conclusion, homozygosity for null variants and nephrocalcinosis were the strongest determinants for kidney failure in PH1.
1型原发性高草酸尿症(PH1)的病程高度异质性。除了c.508G>A(p.Gly170Arg)变异体,其预后相对较好外,关于肾衰竭的决定因素知之甚少。识别这些因素对于疾病管理至关重要,尤其是在这个新疗法的时代。
在这项对纳入OxalEurope登记处的932例PH1患者的回顾性研究中,我们使用生存分析和混合模型分析,分析了基因型-表型相关性以及肾钙质沉着症、尿路结石、尿草酸和乙醇酸排泄对肾衰竭发展的影响。
175例维生素B6无反应性(“无效”)纯合子发生肾衰竭的风险最高,而155例携带c.508G>A和c.454T>A(p.Phe152Ile)变异体的患者风险最低,肾衰竭的中位发病年龄分别为7.8岁和31.8岁。50例携带c.731T>C(p.Ile244Thr)纯合子变异体的患者的肾脏生存率高于无效纯合子(P = 0.003)。在其他可能对维生素B6有反应的变异体患者中发现了不良预后。肾钙质沉着症显著增加了肾衰竭的风险(风险比[HR] 3.17 [2.03 - 4.94],P < 0.001)。分别从117例和87例患者的620份和579份24小时尿液收集中获得了尿草酸和乙醇酸测量值。与乙醇酸不同,随后发生肾衰竭的患者尿草酸排泄更高(P = 0.034)。然而,尿草酸41%的个体内变异导致了较宽的置信区间。
总之,无效变异体纯合性和肾钙质沉着症是PH1中肾衰竭的最强决定因素。