Moermans Vincent R A, Hamers Jan P H, Verbeek Hilde, de Casterlé Bernadette Dierckx, Milisen Koen, Bleijlevens Michel H C
Department of Health Services Research, Care and Public Health Research Institute, Faculty of Health Medicine and Life Sciences, Maastricht University, Duboisdomein 30, Maastricht, 6229 GT, The Netherlands.
Department of Nursing, White Yellow Cross Limburg, Genk, Belgium.
BMC Nurs. 2023 Oct 19;22(1):394. doi: 10.1186/s12912-023-01553-w.
Research shows that half of person(s) living with dementia (PLWD) receive care which they resist and/or have not given consent to, defined as involuntary treatment. District nurses play a key role in providing this care. Knowledge about how district nurses experience involuntary treatment is lacking. Therefore, the aim of this study was to describe the experiences of district nurses who used involuntary treatment for PLWD at home.
A qualitative descriptive design using semi-structured interviews. Sixteen district nurses with experience in involuntary treatment for PLWD were recruited through purposive sampling. Data were analysed using the Qualitative Analysis Guide of Leuven.
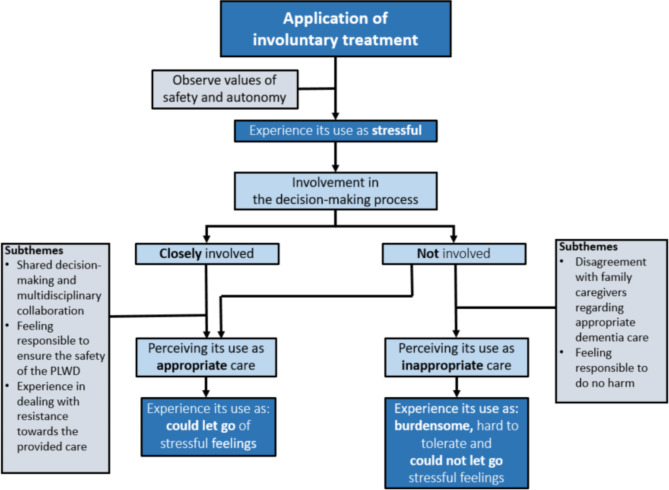
District nurses' experiences with involuntary treatment were influenced by their involvement in the decision-making process. When they were involved, they considered involuntary treatment use to be appropriate care. However, at the moment that involuntary treatment use was started, district nurses were worried that its use was unjust since they wished to respect the wishes of the PLWD. Eventually, district nurses found, from a professional perspective, that involuntary treatment use was necessary, and that safety outweighed the autonomy of the PLWD. District nurses experienced dealing with this dilemma as stressful, due to conflicting values. If district nurses were not involved in the decision-making process regarding the use of involuntary treatment, family caregivers generally decided on its use. Often, district nurses perceived this request as inappropriate dementia care and they first tried to create a dialogue with the family caregivers to reach a compromise. However, in most cases, family caregivers stood by their request and the district nurse still provided involuntary treatment and found this difficult to tolerate.
Our results show that district nurses experience involuntary treatment use as stressful due to dealing with obverse values of safety versus autonomy. To prevent involuntary treatment use and obverse values, we need to increase their ethical awareness, communication skills, knowledge and skills with person-centred care so they can deal with situations that can evolve into involuntary treatment use in a person-centred manner.
研究表明,一半的痴呆症患者(PLWD)接受了他们抗拒和/或未同意的护理,即非自愿治疗。社区护士在提供这种护理方面发挥着关键作用。目前缺乏关于社区护士如何体验非自愿治疗的知识。因此,本研究的目的是描述在家中对痴呆症患者使用非自愿治疗的社区护士的体验。
采用半结构化访谈的定性描述性设计。通过目的抽样招募了16名有对痴呆症患者进行非自愿治疗经验的社区护士。使用鲁汶定性分析指南对数据进行分析。
社区护士对非自愿治疗的体验受到他们参与决策过程的影响。当他们参与其中时,他们认为使用非自愿治疗是适当的护理。然而,在开始使用非自愿治疗的那一刻,社区护士担心其使用是不合理的,因为他们希望尊重痴呆症患者的意愿。最终,社区护士从专业角度发现,使用非自愿治疗是必要的,安全比痴呆症患者的自主权更重要。由于价值观冲突,社区护士在处理这种困境时感到压力很大。如果社区护士没有参与关于使用非自愿治疗的决策过程,家庭照顾者通常会决定是否使用。社区护士通常认为这种要求是不适当的痴呆症护理,他们首先试图与家庭照顾者进行对话以达成妥协。然而,在大多数情况下,家庭照顾者坚持他们的要求,社区护士仍然提供非自愿治疗,并觉得这难以忍受。
我们的结果表明,由于要处理安全与自主权这两种相反的价值观,社区护士在使用非自愿治疗时会感到压力很大。为了防止使用非自愿治疗和处理相反的价值观,我们需要提高他们的道德意识、沟通技巧、以患者为中心的护理知识和技能,以便他们能够以患者为中心的方式处理可能演变为非自愿治疗的情况。