National Clinical Research Center for Cancer/Cancer Hospital, National Cancer Center, Chinese Academy of Medical Sciences and Peking Union Medical College, Beijing, China.
BMC Cancer. 2023 Oct 18;23(1):996. doi: 10.1186/s12885-023-11508-8.
Response of locally advanced gastric cancer (LAGC) to neoadjuvant therapy (NAT) may be associated with prognosis, but which of the clinical or pathological evaluation can accurately predict a favorable prognosis is still controversial. This study aims to compare the effect of clinical and pathological response on the prognosis of patients with gastric cancer.
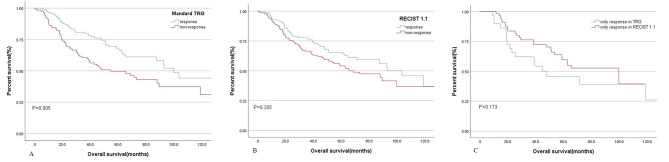
This study retrospectively analyzed LAGC patients who underwent NAT followed by surgery in the China National Cancer Center from January 2004 to January 2021. Clinical and pathological responses after NAT were evaluated using RECIST 1.1 and Mandard tumor regression grade system (TRG) respectively. Complete response (CR) and partial response (PR) assessed by computed tomography were regarded as clinical response. For histopathology regression assessment, response was defined as Mandard 1, 2, 3 and non-response as Mandard 4, 5. Furthermore, we combined clinical and pathological evaluation results into a variable termed "comprehensive assessment" and divided it into four groups based on the presence or absence of response (concurrent response, only clinical response, only pathological response, both non-response). The association between the prognosis and clinicopathological factors was assessed in univariate and multivariate Cox regression analysis.
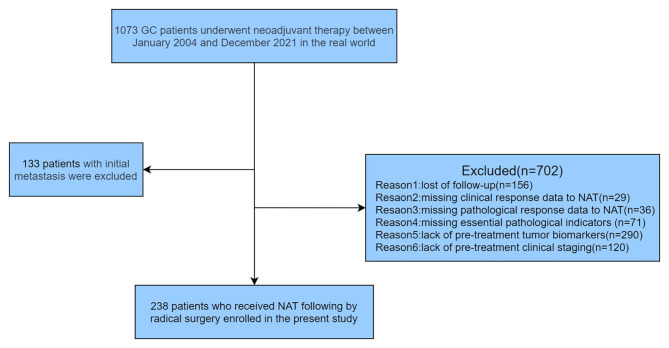
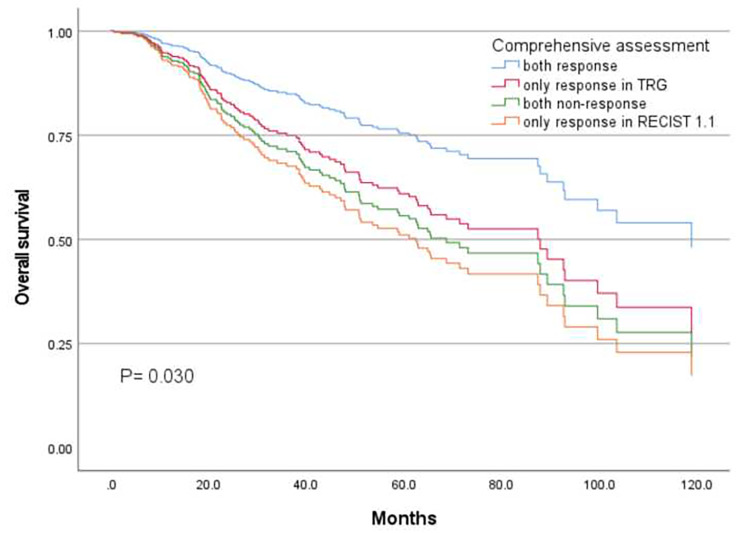
In total, 238 of 1073 patients were included in the study after screening. The postoperative pathological response rate and clinical response rate were 50.84% (121/238) and 39.92% (95/238), respectively. 154 patients got consistent results in clinical and pathological evaluation (66 were concurrent response and 88 were both non-response), while the other 84 patients did not. The kappa value was 0.297(p < 0.001), which showed poor consistency. Multivariate Cox regression analysis revealed that comprehensive assessment (P = 0.03), clinical N stage(P < 0.001), vascular or lymphatic invasion (VOLI) (HR 2.745, P < 0.001), and pre-CA724(HR 1.577, P = 0.047) were independent factors for overall survival in patients with gastric cancer. Among four groups in the comprehensive assessment, concurrent response had significantly better survival (median OS: 103.5 months) than the other groups (P = 0.008).
Concurrent clinical and pathological response might predict a favorable prognosis of patients with gastric cancer after neoadjuvant therapy, further validation is needed in prospective clinical trials with larger samples.
局部晚期胃癌(LAGC)对新辅助治疗(NAT)的反应可能与预后相关,但哪种临床或病理评估能准确预测预后仍存在争议。本研究旨在比较临床和病理反应对胃癌患者预后的影响。
本研究回顾性分析了 2004 年 1 月至 2021 年 1 月在中国国家癌症中心接受 NAT 后手术的 LAGC 患者。分别采用 RECIST 1.1 和 Mandard 肿瘤退缩分级系统(TRG)评估 NAT 后的临床和病理反应。计算机断层扫描评估的完全缓解(CR)和部分缓解(PR)被视为临床反应。对于组织病理学缓解评估,反应定义为 Mandard 1、2、3,非反应定义为 Mandard 4、5。此外,我们将临床和病理评估结果结合起来,形成一个变量,称为“综合评估”,并根据有无反应(同时反应、仅有临床反应、仅有病理反应、均无反应)将其分为四组。单因素和多因素 Cox 回归分析评估了预后与临床病理因素的关系。
经筛选后,共有 1073 例患者中的 238 例纳入本研究。术后病理缓解率和临床缓解率分别为 50.84%(121/238)和 39.92%(95/238)。154 例患者在临床和病理评估中得到了一致的结果(66 例为同时反应,88 例为均无反应),而其余 84 例患者则没有。kappa 值为 0.297(p<0.001),表明一致性较差。多因素 Cox 回归分析显示,综合评估(P=0.03)、临床 N 分期(P<0.001)、血管或淋巴管侵犯(VOLI)(HR 2.745,P<0.001)和术前 CA724(HR 1.577,P=0.047)是胃癌患者总生存的独立因素。在综合评估的四组中,同时反应的患者具有显著更好的生存(中位 OS:103.5 个月),优于其他组(P=0.008)。
同时出现临床和病理缓解可能预测接受新辅助治疗的胃癌患者有良好的预后,需要更大样本量的前瞻性临床试验进一步验证。