Department of Neurology, Yantai Yuhuangding Hospital Affiliated to Qingdao University, No. 20 East Yuhuangding Road, Yantai, 264000, Shandong, China.
Yantai Regional Sub-Center of China National Clinical Research Center for Neurological Diseases, Yantai, China.
Eur J Med Res. 2023 Oct 19;28(1):446. doi: 10.1186/s40001-023-01445-4.
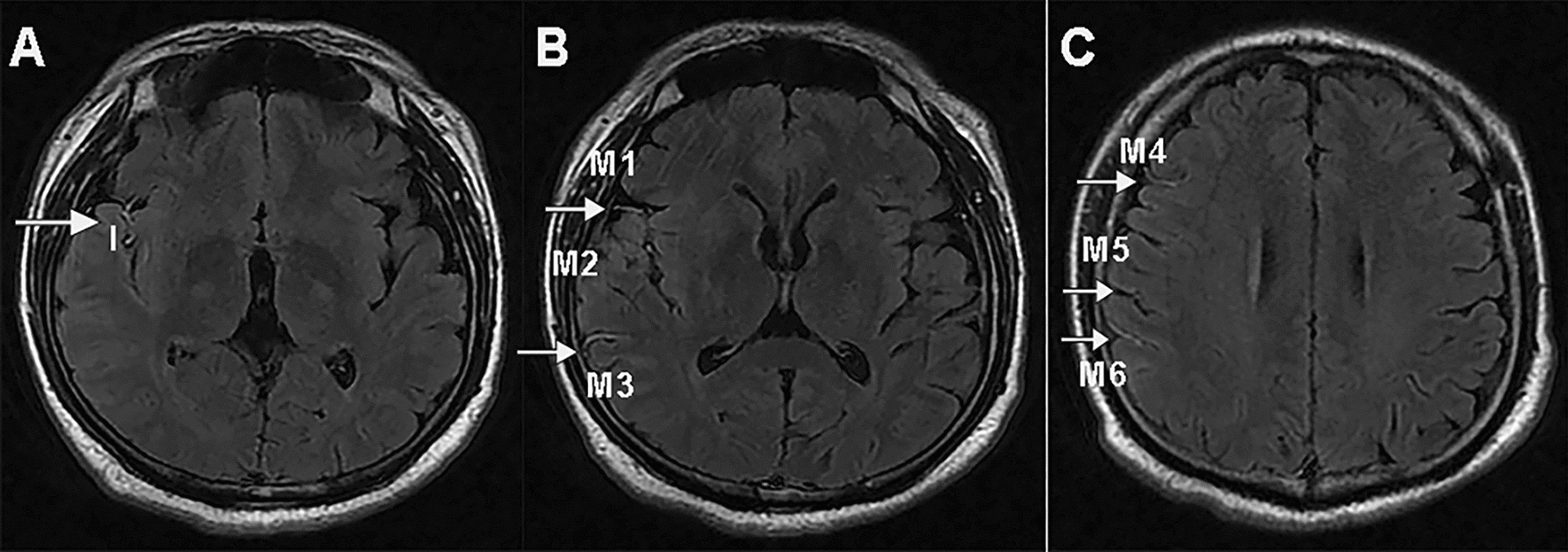
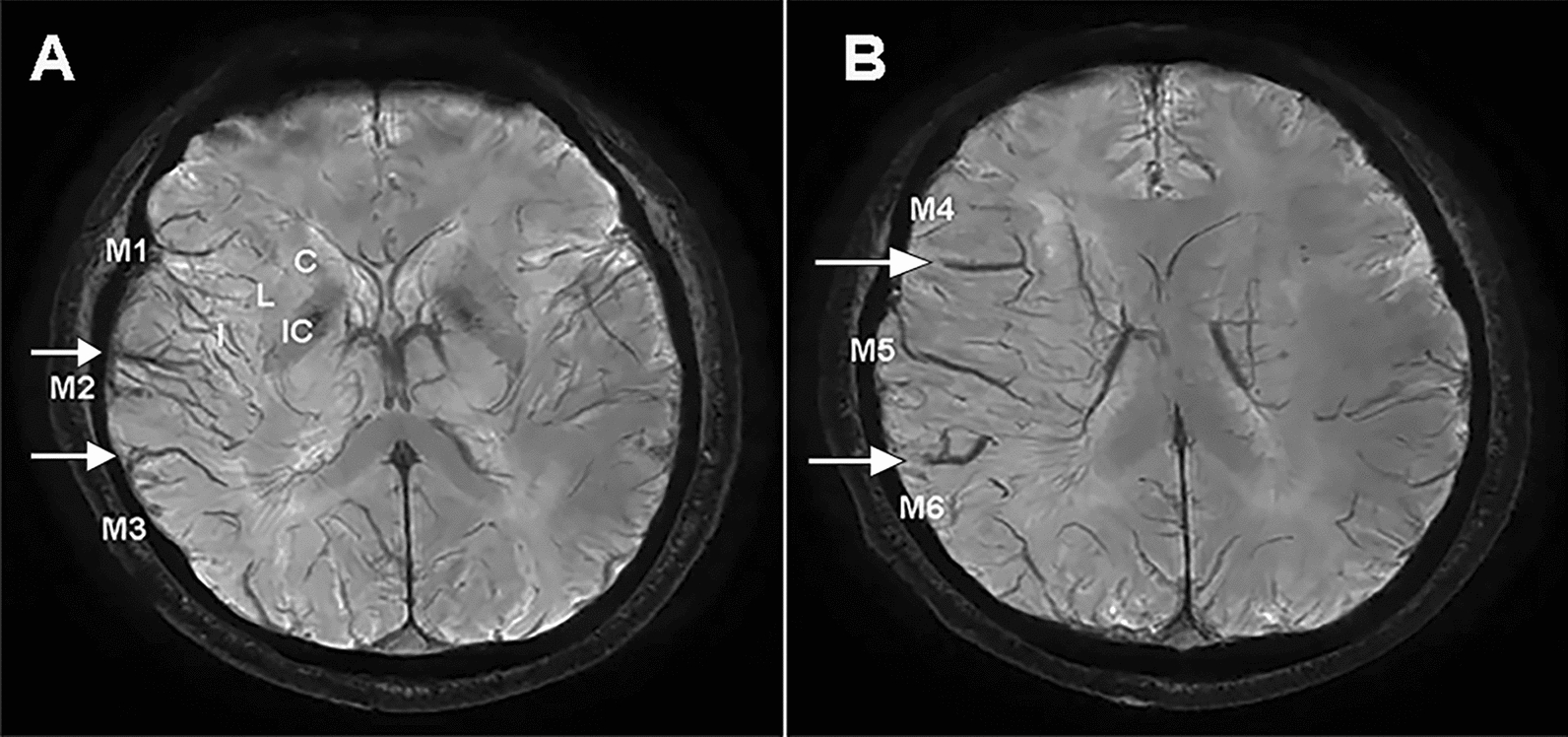
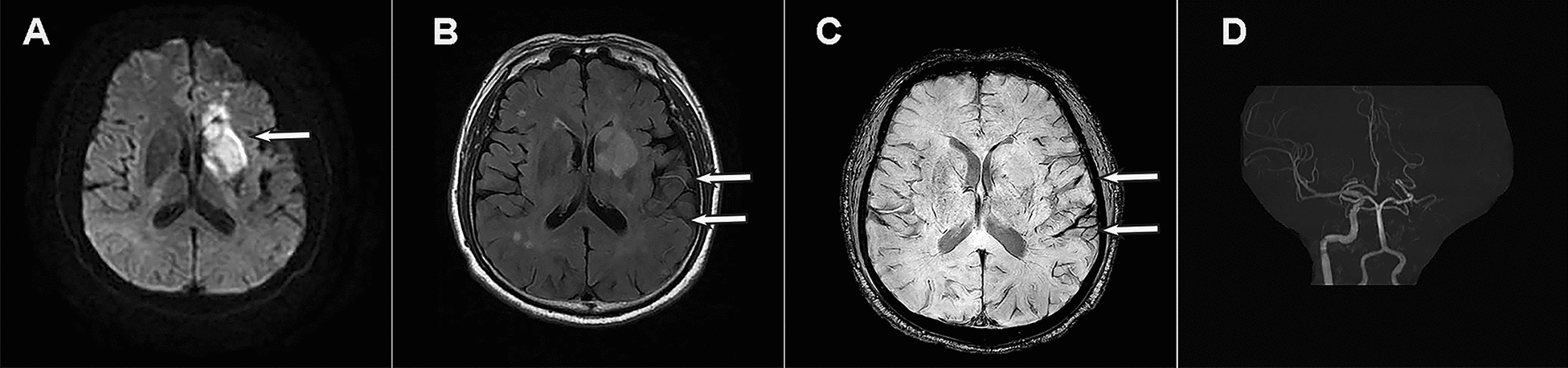
To investigate the value of fluid-attenuated inversion recovery vascular hyperintensity (FVH) within asymmetrical prominent veins sign (APVS) on susceptibility-weighted imaging predicting collateral circulation and prognosis in patients with acute anterior circulation ischemic stroke.
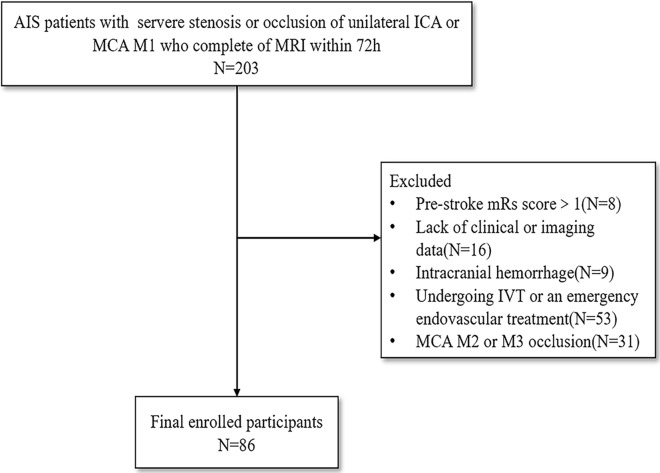
Patients with severe stenosis or occlusion of ICA or MCA M1, who underwent MRI within 72 h from stroke onset were reviewed. The Alberta Stroke Program Early CT Score was used to evaluate the volume of infarction on DWI, the degree of FVH and APVS. Spearman correlation analysis was used to evaluate the correlation between FVH and APVS. All patients were divided into the good prognosis group and the poor prognosis group according to the score of the modified ranking scale (mRS) 90 days after the stroke. Logistic regression analysis was used to explore the relationship between FVH and APVS and functional prognosis, while receiver operating characteristic (ROC) curves were plotted to assess the value of FVH and APVS in predicting prognosis.
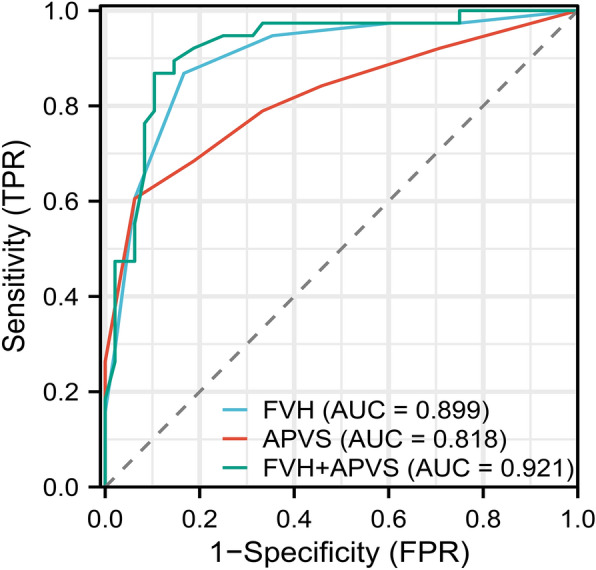
Spearman correlation analysis revealed moderate positive correlations between FVH and APVS (r = 0.586, P < 0.001). The poor prognosis group had a higher rate of a history of atrial fibrillation, a larger cerebral infarction volume, a higher NIHSS score at admission, and a higher FVH and APVS score compared with the good prognosis group (all P < 0.05). A further logistic regression indicated that the NIHSS score, cerebral infarction volume, FVH and APVS were independent risk factors for a poor functional prognosis. In terms of FVH, APVS, alone and their combination for the diagnosis of poor prognosis, the sensitivity, specificity, area under the ROC curve (AUC), and 95% confidence interval (CI) were 86.8%, 83.3%, 0.899 (95% CI 0.830-0.968); 60.5%, 93.7%, 0.818 (95% CI 0.723-0.912); 86.8%, 89.6%, 0.921 (95% CI 0.860-0.981), respectively.
The presence of FVH and APVS can provide a comprehensive assessment of collateral circulation from the perspective of veins and arteries, and the correlation between the two is positively correlated. Both of them were independent risk factors for poor prognosis, their combination is complementary and can improve the predictive value.
本研究旨在探讨磁敏感加权成像(SWI)不对称突出静脉征(APVS)内液衰减反转恢复血管高信号(FVH)在预测急性前循环缺血性卒中患者侧支循环和预后中的价值。
回顾性分析了发病后 72 小时内行 MRI 检查的颈内动脉(ICA)或大脑中动脉 M1 重度狭窄或闭塞患者。采用 Alberta 卒中项目早期 CT 评分(ASPECTS)评估 DWI 上梗死体积,FVH 和 APVS 程度。采用 Spearman 相关分析评估 FVH 和 APVS 之间的相关性。所有患者根据发病 90 天后改良 Rankin 量表(mRS)评分分为预后良好组和预后不良组。采用 Logistic 回归分析探讨 FVH 和 APVS 与功能预后的关系,绘制受试者工作特征(ROC)曲线评估 FVH 和 APVS 预测预后的价值。
Spearman 相关分析显示 FVH 和 APVS 之间存在中度正相关(r=0.586,P<0.001)。与预后良好组相比,预后不良组中心房颤动史、脑梗死体积较大、入院时 NIHSS 评分较高、FVH 和 APVS 评分较高的比例较高(均 P<0.05)。进一步的 Logistic 回归分析表明,NIHSS 评分、脑梗死体积、FVH 和 APVS 是功能预后不良的独立危险因素。就 FVH、APVS 单独及两者联合诊断预后不良而言,其灵敏度、特异度、ROC 曲线下面积(AUC)及 95%置信区间(CI)分别为 86.8%、83.3%、0.899(95%CI 0.830-0.968);60.5%、93.7%、0.818(95%CI 0.723-0.912);86.8%、89.6%、0.921(95%CI 0.860-0.981)。
FVH 和 APVS 的存在可以从静脉和动脉两个方面全面评估侧支循环,两者呈正相关。它们都是预后不良的独立危险因素,两者联合具有互补性,可以提高预测价值。