Abbruzzese Chiara, Guzzardella Amedeo, Consonni Dario, Turconi Gloria, Bonetti Claudia, Brioni Matteo, Panigada Mauro, Grasselli Giacomo
Department of Anaesthesiology, Critical Care and Emergency, Intensive Care and Emergency, Fondazione IRCCS Ca' Granda Ospedale Maggiore Policlinico, Via Francesco Sforza, 35, 20122, Milan, Italy.
Department of Pathophysiology and Transplantation, University of Milan, Via Francesco Sforza, 35, 20122, Milan, Italy.
Ann Intensive Care. 2023 Oct 19;13(1):106. doi: 10.1186/s13613-023-01206-w.
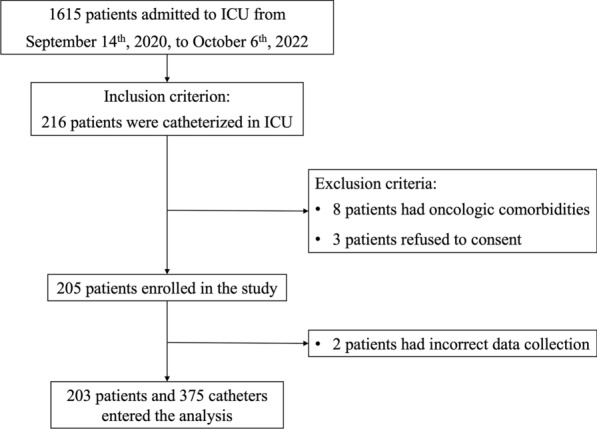
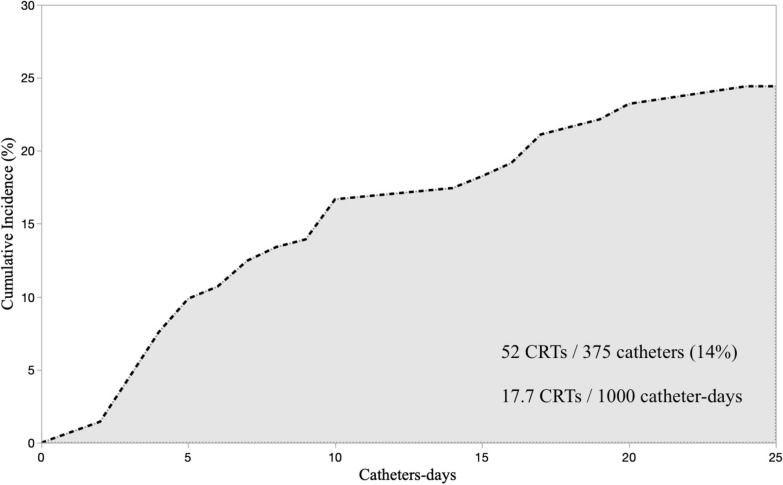
Catheter-related thrombosis (CRT) incidence, rate, and risk factors vary in literature due to differences in populations, catheters, diagnostic methods, and statistical approaches. The aim of this single-center, prospective, observational study was to assess incidence, incidence rate (IR), cumulative incidence, and risk factors by means of IR ratio (IRR) of asymptomatic CRT in a non-oncologic Intensive Care Unit (ICU) population. CRT development was assessed daily by means of ultrasound screening. The proportions of patients and catheters developing CRT and CRT incidence rates, expressed as the number of events per catheter-days (cd), were calculated. Kalbfleisch and Prentice's method was used to estimate the cumulative incidence of CRTs. Univariate and multivariable Poisson regression models were fitted to calculate IRR in risk factors analysis.
Fifty (25%, 95% CI 19-31) out of 203 included patients, and 52 (14%, 95% CI 11-18) out of 375 catheters inserted developed CRT [IR 17.7 (13.5-23.2) CRTs/1000cd], after 5 [3-10] days from insertion. Forty-six CRTs (88%) were partial thrombosis. All CRTs remained asymptomatic. Obesity and ECMO support were patient-related protective factors [IRR 0.24 (0.10-0.60), p = 0.002 and 0.05 (0.01-0.50), p = 0.011, respectively]. The internal jugular vein had higher CRT IR than other sites [20.1 vs. 5.9 CRTs/1000cd, IRR 4.22 (1.22-14.63), p = 0.023]. Pulmonary artery catheter and left-side cannulation were catheter-related risk factors [IRR 4.24 (2.00-9.00), p < 0.001 vs. central venous catheters; IRR 2.69 (1.45-4.98), p = 0.002 vs. right cannulation, respectively]. No statistically significant effect of the number of simultaneously inserted catheters [IRR 1.11 (0.64-1.94), p = 0.708] and of the catheterization length [IRR 1.09 (0.97-1.22), p = 0.155] was detected. The ICU length of stay was longer in CRT patients (20 [15-31] vs. 6 [4-14] days, p < 0.001), while no difference in mortality was observed.
CRTs are frequent but rarely symptomatic. This study suggests that obesity and ECMO are protective factors, while pulmonary artery catheter, internal jugular vein and left-side positioning are risk factors for CRT.
由于研究人群、导管、诊断方法和统计方法的差异,文献中导管相关血栓形成(CRT)的发生率、发病率及危险因素各不相同。本单中心、前瞻性、观察性研究旨在通过非肿瘤重症监护病房(ICU)人群中无症状CRT的发病率比(IRR)来评估其发生率、发病率、累积发病率及危险因素。通过超声筛查每日评估CRT的发生情况。计算发生CRT的患者和导管比例以及CRT发病率,以每导管日(cd)的事件数表示。采用卡尔弗莱施和普伦蒂斯方法估计CRT的累积发病率。在危险因素分析中,采用单变量和多变量泊松回归模型计算IRR。
203例纳入患者中有50例(25%,95%CI 19 - 31),375根插入导管中有52根(14%,95%CI 11 - 18)发生CRT [发病率为17.7(13.5 - 23.2)例CRT/1000cd],发生在插入导管后5 [3 - 10]天。46例CRT(88%)为部分血栓形成。所有CRT均无症状。肥胖和体外膜肺氧合(ECMO)支持是与患者相关的保护因素[IRR分别为0.24(0.10 - 0.60),p = 0.002和0.05(0.01 - 0.50),p = 0.011]。颈内静脉的CRT发病率高于其他部位[20.1 vs. 5.9例CRT/1000cd,IRR 4.22(1.22 - 14.63),p = 0.023]。肺动脉导管和左侧置管是与导管相关的危险因素[与中心静脉导管相比,IRR 4.24(2.00 - 9.00),p < 0.001;与右侧置管相比,IRR 2.69(1.45 - 4.98),p = 0.002]。未检测到同时插入导管数量[IRR 1.11(0.64 - 1.94),p = 0.708]和置管长度[IRR 1.09(0.97 - 1.22),p = 0.155]的统计学显著影响。CRT患者的ICU住院时间更长(20 [15 - 31]天 vs. 6 [4 - 14]天,p < 0.001),但死亡率无差异。
CRT很常见,但很少有症状。本研究表明肥胖和ECMO是保护因素,而肺动脉导管、颈内静脉和左侧置管是CRT的危险因素。