Division of Pulmonology and Critical Care Medicine, Department of Internal Medicine, Nowon Eulji Medical Center, University of Eulji, Seoul, South Korea.
Department of Anesthesiology and Pain Medicine, Asan Medical Center, Ulsan College of Medicine, Seoul, South Korea.
BMC Pulm Med. 2023 Oct 20;23(1):400. doi: 10.1186/s12890-023-02700-4.
Tuberculous effusion varies from lymphocyte-dominant to neutrophilic effusion according to inflammation status. The criteria of adenosine deaminase (ADA) and lymphocyte/neutrophil (L/N) ratio have yet not been evaluated across different disease conditions.
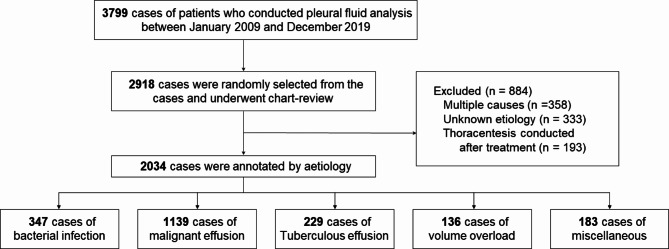
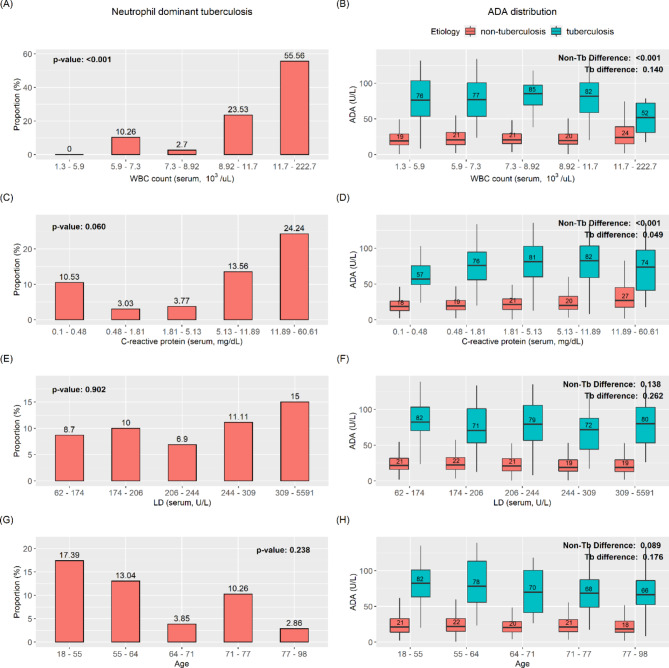
Patients who conducted pleural fluid analysis from 2009 to 2019 at Asan Medical Center were included. Criteria (ADA of 50 and L/N ratio of 0.75) were evaluated by quantile subgroups according to age, C-reactive protein (CRP), white blood cell (WBC), and lactate dehydrogenase (LD) by the Monte Carlo simulation method to diagnose tuberculosis. The model for the ADA and L/N ratio was evaluated by AUROC.
Among the 2,918 reviewed cases, 2034 were included with 229 (11.26%) tuberculosis cases. The mean baseline ADA AUROC was 0.88 across all patients. Increased CRP and WBC showed high proportions of neutrophilic tuberculous effusion, with low sensitivity of approximately 45% and 33% in the fifth WBC and CRP groups, respectively. The AUROC of the models decreased with the increase in WBC and CRP groups (ADA model: 0.69 [the top quantile WBC group], 0.74 [the top quantile CRP group]). The AUROC of the models did not show a trend according to the increase in LD and age.
Inflammatory status affects the diagnostic metrics for tuberculous effusion due to the progression of tuberculous effusion. Clinicians should consider the low accuracy of tuberculous effusion criteria in high-inflammatory conditions when diagnosing tuberculosis.
根据炎症状态,结核性渗出液可从淋巴细胞为主变为中性粒细胞为主。腺苷脱氨酶(ADA)和淋巴细胞/中性粒细胞(L/N)比值的标准尚未在不同疾病情况下进行评估。
纳入 2009 年至 2019 年在 Asan 医疗中心进行胸腔积液分析的患者。通过蒙特卡罗模拟方法,根据年龄、C 反应蛋白(CRP)、白细胞(WBC)和乳酸脱氢酶(LD)的分位数亚组评估 ADA 为 50 和 L/N 比为 0.75 的标准,以诊断结核病。通过 AUROC 评估 ADA 和 L/N 比值模型。
在 2918 例回顾性病例中,纳入 2034 例,其中 229 例(11.26%)为结核病病例。所有患者的 ADA 基线 AUROC 的平均值为 0.88。CRP 和 WBC 升高表明存在中性粒细胞为主的结核性渗出液,敏感性分别约为 45%和 33%,在第五个 WBC 和 CRP 组中。随着 WBC 和 CRP 组的增加,模型的 AUROC 降低(ADA 模型:WBC 最高分位数组为 0.69,CRP 最高分位数组为 0.74)。随着 LD 和年龄的增加,模型的 AUROC 没有显示出趋势。
由于结核性渗出液的进展,炎症状态会影响结核性渗出液的诊断指标。临床医生在诊断结核病时,应考虑到高炎症状态下结核性渗出液标准的准确性较低。