Division of Pulmonary and Critical Care Medicine, Department of Internal Medicine, Incheon St. Mary's Hospital, College of Medicine, The Catholic University of Korea, Seoul, Republic of Korea.
Incheon Baek Hospital, Incheon, Republic of Korea.
Sci Rep. 2022 May 9;12(1):7586. doi: 10.1038/s41598-022-11460-w.
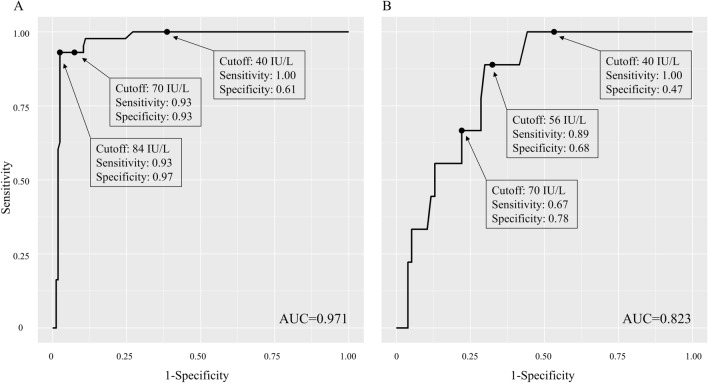
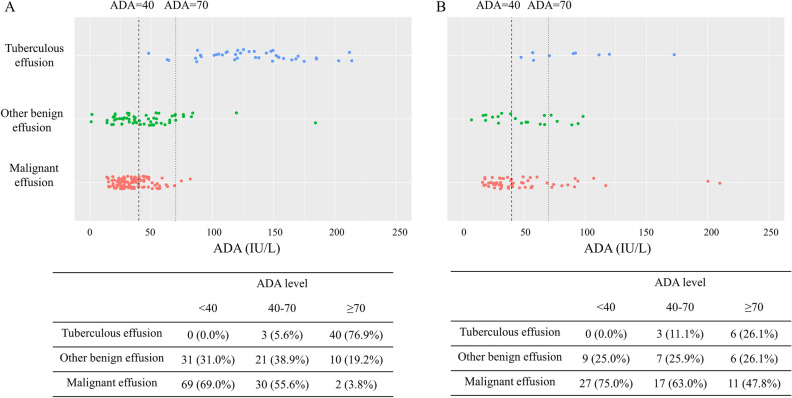
As the burden of tuberculosis (TB) in South Korea decreases while that of malignancy increases with an aging society, the composition of etiology for pleural effusion is changing. The aim of this study was to investigate the diagnostic value of adenosine deaminase (ADA) for diagnosis of tuberculous pleural effusion (TPE) in this circumstance. Medical records of patients who underwent medical thoracoscopy from May 2015 to September 2020 in Incheon St. Mary Hospital, Korea were retrospectively reviewed. TPE was diagnosed if one of the following criteria was met: (1) granuloma in pleura, (2) positive TB polymerase chain reaction or culture in pleural fluid or tissue with non-specific pathologic findings in pleura, or (3) bacteriologically confirmed pulmonary TB with non-specific pathologic findings in pleura. A total of 292 patients, including 156 with malignant pleural effusion (MPE), 52 with TPE, and 84 with other benign effusion, were analyzed. Among 206 patients with lymphocyte dominant pleural effusion, the area under receiver characteristic curve of ADA for diagnosis of TPE was 0.971. The sensitivity and specificity of a current cutoff value of 40 IU/L were 1.00 and 0.61, respectively, whereas those of a raised cutoff value of 70 IU/L were 0.93 and 0.93, respectively. Among 54 patients with ADA levels of 40-70 IU/L, 30 (55.6%) patients were diagnosed as MPE, 21 (38.9%) as other benign effusion, and only 3 (5.6%) as TPE. Caution is needed in clinical diagnosis of TPE with current ADA cutoff value in countries with decreasing TB incidence, due to many false positive cases.
随着韩国结核病(TB)负担的减少,以及老龄化社会恶性肿瘤负担的增加,胸腔积液的病因构成正在发生变化。本研究旨在探讨腺苷脱氨酶(ADA)在这种情况下对结核性胸腔积液(TPE)诊断的诊断价值。回顾性分析了 2015 年 5 月至 2020 年 9 月在韩国仁川圣玛丽医院接受胸腔镜检查的患者的病历。如果符合以下标准之一,则诊断为 TPE:(1)胸膜肉芽肿;(2)胸腔液或组织中结核聚合酶链反应或培养阳性,或胸膜非特异性病理发现;(3)有非特异性病理发现的细菌性肺结核合并胸腔积液。共分析了 292 例患者,其中 156 例为恶性胸腔积液(MPE),52 例为 TPE,84 例为其他良性胸腔积液。在 206 例淋巴细胞优势性胸腔积液患者中,ADA 诊断 TPE 的受试者工作特征曲线下面积为 0.971。目前 40 IU/L 截断值的灵敏度和特异性分别为 1.00 和 0.61,而升高的 70 IU/L 截断值的灵敏度和特异性分别为 0.93 和 0.93。在 ADA 水平为 40-70 IU/L 的 54 例患者中,30 例(55.6%)诊断为 MPE,21 例(38.9%)为其他良性胸腔积液,仅 3 例(5.6%)为 TPE。在结核病发病率下降的国家,由于许多假阳性病例,目前的 ADA 截断值在 TPE 的临床诊断中需要谨慎。