Cole Kyril L, Boehme Amelia K, Thacker Evan L, Longstreth W T, Brown Bruce L, Gale Shawn D, Hedges Dawson W, Anderson Jacqueline K, Elkind Mitchell S V
School of Medicine, University of Utah, Salt Lake City, Utah, USA,
Department of Epidemiology, Mailman School of Public Health, Columbia University, New York, New York, USA.
Cerebrovasc Dis. 2024;53(4):382-390. doi: 10.1159/000533568. Epub 2023 Oct 23.
Hospital-acquired infections (HAIs) after stroke are associated with additional morbidity and mortality, but whether HAIs increase long-term cognitive decline in stroke patients is unknown. We hypothesized that older adults with incident stroke with HAI experience faster cognitive decline than those having stroke without HAI and those without stroke.
We performed a longitudinal analysis in the population-based prospective Cardiovascular Health Study. Medicare-eligible participants aged ≥65 years with and without incident stroke had cognition assessed annually. HAIs were assessed by hospital discharge codes. Global cognitive function was assessed annually by the Modified Mini-Mental State Examination (3MSE) and executive function by the Digit Symbol Substitution Test (DSST). We used linear mixed models to estimate the mean decline and 95% confidence intervals (95% CI) for 3MSE and DSST scores by incident stroke and HAI status, adjusted for demographics and vascular risk factors.
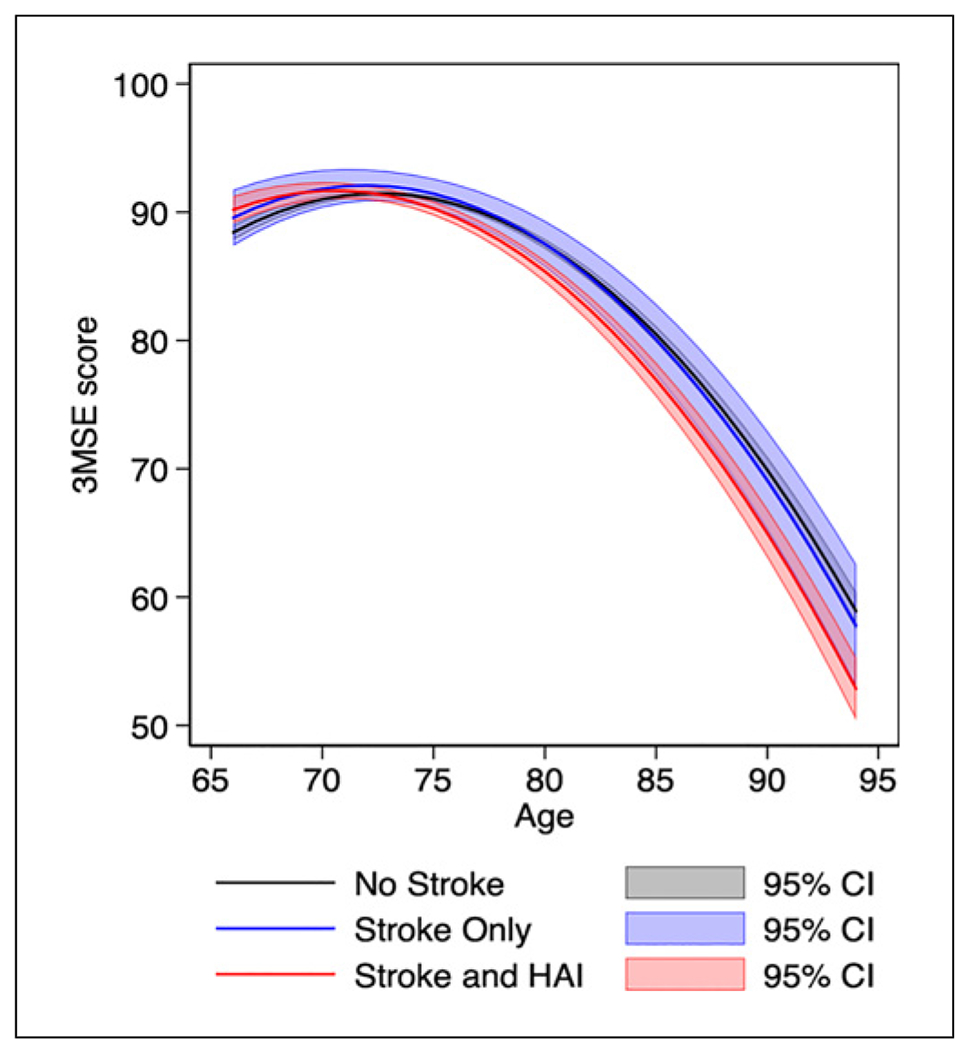
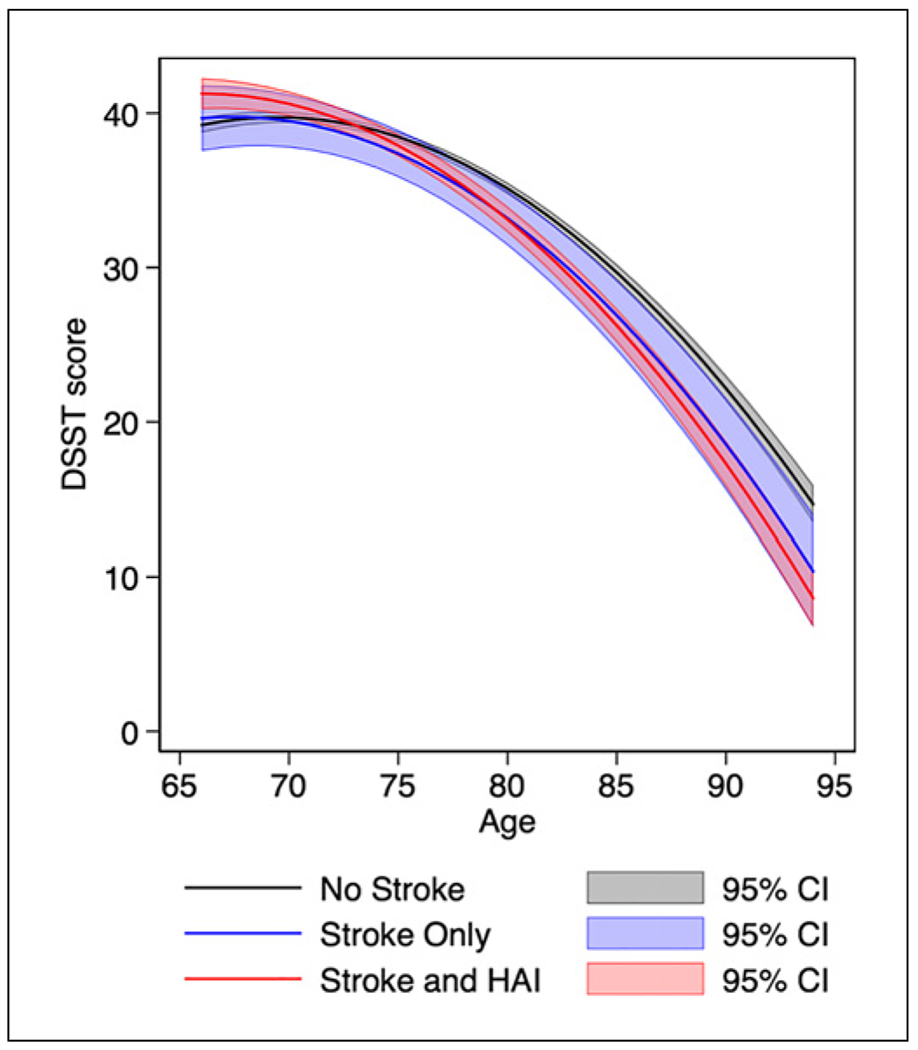
Among 5,443 participants ≥65 years without previous history of stroke, 393 participants had stroke with HAI (SI), 766 had a stroke only (SO), and 4,284 had no stroke (NS) throughout a maximum 9-year follow-up. For 3MSE, compared with NS participants, SO participants had a similar adjusted mean decline (additional 0.08 points/year, 95% CI: -0.15, 0.31), while SI participants had a more rapid decline (additional 0.28 points/year, 95% CI: 0.16, 0.40). Adjusted mean decline was 0.20 points/year faster (95% CI: -0.05, 0.45) among SI than SO participants. For DSST, compared with NS participants, SO participants had a faster adjusted mean decline (additional 0.17 points/year [95% CI: 0.003, 0.33]), as did SI participants (additional 0.27 points/year [95% CI: 0.19, 0.35]).
Stroke, when accompanied by HAI, leads to a faster long-term decline in cognitive ability than in those without stroke. The clinical and public health implications of the effect of infection on post-stroke cognitive decline warrant further attention.
卒中后医院获得性感染(HAIs)与额外的发病率和死亡率相关,但HAIs是否会增加卒中患者的长期认知功能衰退尚不清楚。我们假设发生卒中且伴有HAIs的老年人比未发生卒中以及发生卒中但未伴有HAIs的老年人认知功能衰退更快。
我们在基于人群的前瞻性心血管健康研究中进行了一项纵向分析。年龄≥65岁且符合医疗保险资格的有或无卒中事件的参与者每年接受认知评估。HAIs通过医院出院编码进行评估。每年通过改良简易精神状态检查(3MSE)评估整体认知功能,通过数字符号替换测验(DSST)评估执行功能。我们使用线性混合模型,根据卒中事件和HAIs状态估计3MSE和DSST分数的平均衰退及95%置信区间(95%CI),并对人口统计学和血管危险因素进行了调整。
在5443名年龄≥65岁且无卒中既往史的参与者中,在最长9年的随访期间,393名参与者发生了伴有HAIs的卒中(SI),766名仅发生了卒中(SO),4284名未发生卒中(NS)。对于3MSE,与NS参与者相比,SO参与者调整后的平均衰退相似(每年额外衰退0.08分,95%CI:-0.15,0.31),而SI参与者衰退更快(每年额外衰退0.28分,95%CI:0.16,0.40)。SI参与者的调整后平均衰退比SO参与者每年快0.20分(95%CI:-0.05,0.45)。对于DSST,与NS参与者相比,SO参与者调整后的平均衰退更快(每年额外衰退0.17分[95%CI:0.003,0.33]),SI参与者也是如此(每年额外衰退0.27分[95%CI:0.19,0.35])。
卒中伴有HAIs时,导致的认知能力长期衰退比未发生卒中时更快。感染对卒中后认知衰退影响的临床和公共卫生意义值得进一步关注。