Obra Jed Keenan, Lin Bryant, Đoàn Lan N, Palaniappan Latha, Srinivasan Malathi
Stanford Center for Asian Research and Education, Stanford University School of Medicine; Palo Alto, CA.
Department of Neurobiology, Physiology, and Behavior, University of California Davis; Davis, CA.
J Asian Health. 2021 Jul;1(1). doi: 10.59448/jah.v1i1.3. Epub 2021 Jul 14.
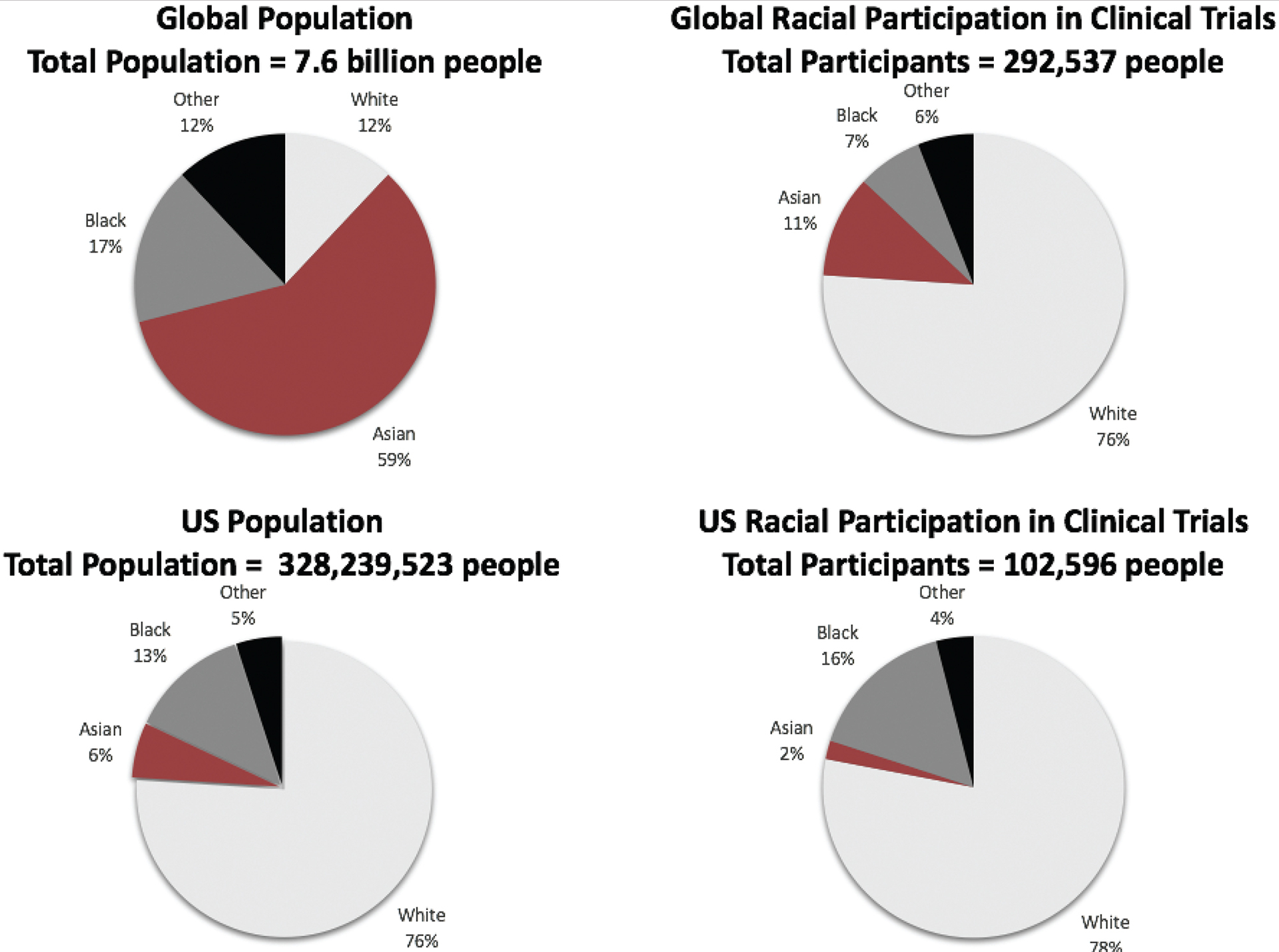
Equity is a fundamental goal of the US health care system. Asians comprise 6% of the US population, and 60% of the world's population. Less than 1% of National Institutes of Health funding is directed toward Asian health. Asian health outcomes are often worse than non-Hispanic Whites (NHWS) in America. Increasing federal and foundation resources and funding toward Asian health research could illuminate these risks and develop precision interventions to reduce known health disparities. When disaggregated by race/ethnicity, Asian health risks are even more apparent. Here, we discuss critical health outcome differences between the six major Asian American subgroups (Asian Indian, Chinese, Filipino, Japanese, Korean, and Vietnamese) comprising 80% of the US Asian population, highlighting demographic, pharmacologic, disease prevalence, and mortality outcomes. We then outline seven critical issues contributing to Asian American health disparities, including aggregated Asian health data, undersampling, invalid extrapolations, underrepresentation in clinical trials, lack of funding and awareness of disparities, and the model minority myth. Building on the successes of national public health initiatives, we propose nine leverage points to improve Asian American health including the following: obtaining disaggregated Asian health data, improved Asian health research (oversampling Asians, improving clinical trial participation, and increasing research funding), stakeholder collaboration (national and with Asian nations), community engagement, providing culturally precise health care, and expansion of the Asian American research ecosystem. Achieving health equity takes deliberate practice and does not occur by accident. By addressing critical issues that perpetuate Asian health disparities, we grow closer to understanding how to effectively improve Asian health and build a nationally unified mindset toward action that emphasizes equitable care for all.
公平是美国医疗保健系统的一个基本目标。亚洲人占美国人口的6%,占世界人口的60%。美国国立卫生研究院的资金中,用于亚洲人健康研究的不到1%。在美国,亚洲人的健康结果往往比非西班牙裔白人更差。增加联邦和基金会对亚洲人健康研究的资源和资金投入,可能会揭示这些风险,并开发精准干预措施以减少已知的健康差距。按种族/族裔细分时,亚洲人的健康风险更加明显。在这里,我们讨论了占美国亚洲人口80%的六个主要亚裔美国人群体(印度裔、华裔、菲律宾裔、日裔、韩裔和越南裔)之间关键的健康结果差异,重点介绍了人口统计学、药理学、疾病患病率和死亡率结果。然后,我们概述了导致亚裔美国人健康差距的七个关键问题,包括汇总的亚洲人健康数据、抽样不足、无效推断、在临床试验中代表性不足、缺乏资金以及对差距的认识不足,以及模范少数族裔神话。基于国家公共卫生倡议的成功经验,我们提出了九个改善亚裔美国人健康的杠杆点,包括以下几点:获取细分的亚洲人健康数据、改进亚洲人健康研究(对亚洲人进行过度抽样、提高临床试验参与度以及增加研究资金)、利益相关者合作(国内和与亚洲国家)、社区参与、提供文化精准的医疗保健,以及扩大亚裔美国人研究生态系统。实现健康公平需要深思熟虑的实践,而不是偶然发生的。通过解决导致亚洲人健康差距长期存在的关键问题,我们更接近于了解如何有效地改善亚洲人的健康,并建立一种全国统一的行动思维模式,强调为所有人提供公平的医疗保健。