Mirunalini Gunaseelan, Anand Kuppusamy, Pushparani Anand, Kadirvelu Gunasri
Anesthesiology, SRM (Sri Ramaswamy Memorial) Medical College Hospital and Research Centre, Chennai, IND.
Cureus. 2023 Sep 22;15(9):e45798. doi: 10.7759/cureus.45798. eCollection 2023 Sep.
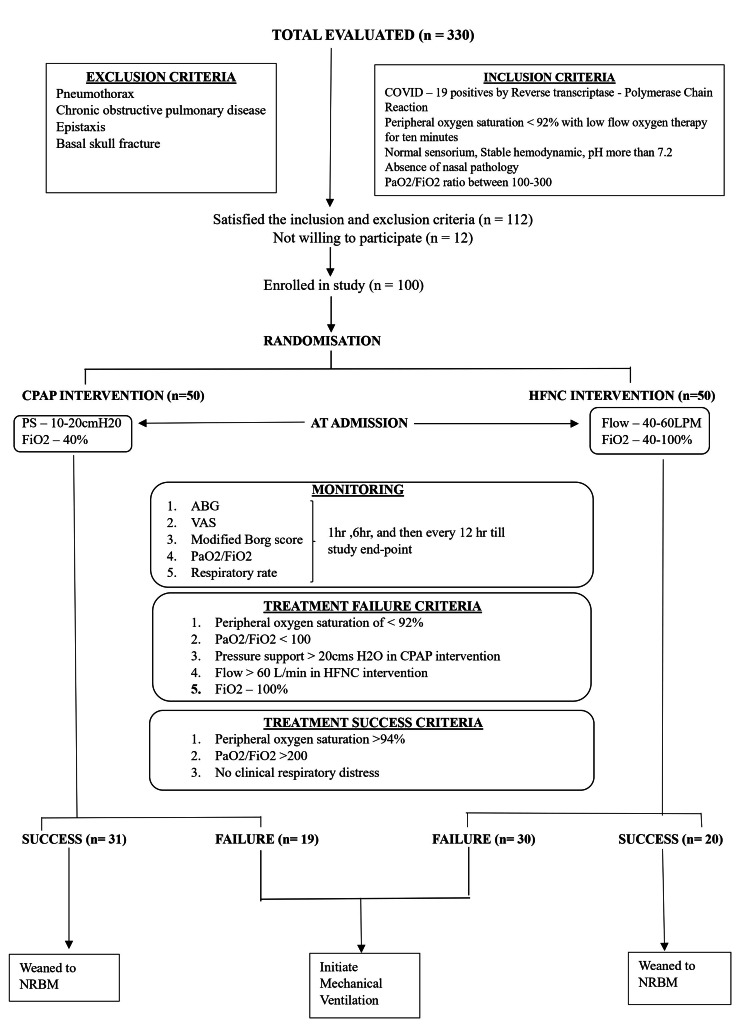
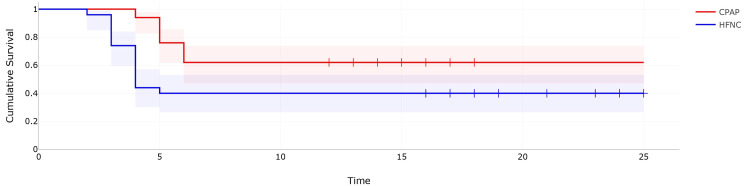
Background and objective Acute hypoxic respiratory failure in coronavirus disease 2019 (COVID-19) pneumonia has been treated with oxygen delivered by oxygen masks and non-invasive ventilation (NIV) with continuous positive airway pressure (CPAP), and more recently with high-flow nasal cannula (HFNC) devices. There is a paucity of randomized controlled trials to compare the efficacy of CPAP with HFNC in COVID-19 pneumonia. We conceptualized a randomized control study to compare the efficacy of HFNC and CPAP in reducing the need for invasive mechanical ventilation, estimation of mechanical ventilation-free days, and risk of intubation in COVID-19 patients with hypoxic respiratory failure. Methodology One hundred consecutive patients who satisfied the inclusion criteria were included in the trial. The patients were then randomly allocated to receive either CPAP or HFNC with settings as per the study protocol. The patients were deemed to have achieved the study endpoint when they were intubated due to any reason or successfully weaned from NIV to conventional oxygen therapies. The number of patients who required invasive ventilation and the number of invasive ventilation-free days were recorded and analyzed. Results Nineteen (38%) patients in the CPAP group and 30 (60%) patients in the HFNC group required invasive mechanical ventilation and the difference was statistically significant (p = 0.03, 95%CI: 0.1829-0.9129). The median number of days free of invasive mechanical ventilation in the CPAP group (median=5 (interquartile range (IQR(=5,6)) was more than in the HFNC group (median=4 (IQR=3,4)) and this difference was statistically significant (p<0.000). The secondary analysis of risk evaluation for intubation done using the Cox regression model showed no significant factors that could have contributed to intubation in the study population. The Kaplan-Meyer curve was used to express the probability of a patient getting intubated and the calculated hazard ratio was 2.29. Conclusion The administration of CPAP significantly reduced the intubation rate and prolonged invasive mechanical ventilation-free period in COVID-19 patients with hypoxic respiratory failure. We also inferred a two-fold increase in the risk of intubation in patients receiving HFNC compared to CPAP.
背景与目的 2019 冠状病毒病(COVID-19)肺炎所致的急性低氧性呼吸衰竭,一直采用面罩吸氧和持续气道正压通气(CPAP)的无创通气进行治疗,最近也开始使用高流量鼻导管(HFNC)设备。比较 CPAP 与 HFNC 治疗 COVID-19 肺炎疗效的随机对照试验较少。我们构思了一项随机对照研究,以比较 HFNC 和 CPAP 在减少 COVID-19 低氧性呼吸衰竭患者有创机械通气需求、评估无机械通气天数以及插管风险方面的疗效。
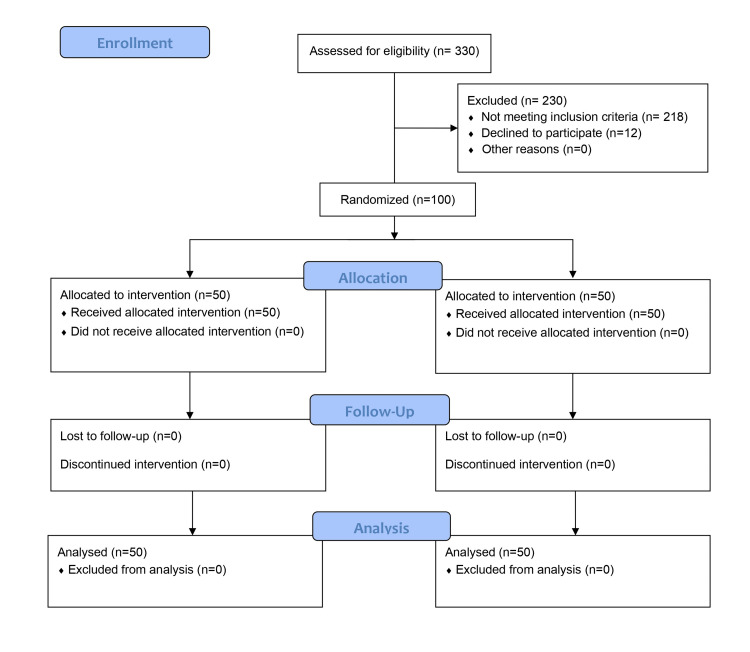
方法 连续纳入 100 例符合纳入标准的患者进行试验。然后根据研究方案,将患者随机分配接受 CPAP 或 HFNC 治疗。当患者因任何原因插管或成功从无创通气撤机改为传统氧疗时,视为达到研究终点。记录并分析需要有创通气的患者数量和无有创通气天数。
结果 CPAP 组 19 例(38%)患者和 HFNC 组 30 例(60%)患者需要有创机械通气,差异有统计学意义(p = 0.03,95%CI:0.1829 - 0.9129)。CPAP 组无有创机械通气的中位天数(中位数 = 5(四分位间距(IQR)= 5,6))多于 HFNC 组(中位数 = 4(IQR = 3,4)),且差异有统计学意义(p < 0.000)。使用 Cox 回归模型对插管风险评估进行的二次分析显示,研究人群中没有显著因素可导致插管。采用 Kaplan - Meyer 曲线表示患者插管的概率,计算得出的风险比为 2.29。
结论 在 COVID-19 低氧性呼吸衰竭患者中,CPAP 治疗显著降低了插管率,延长了无有创机械通气期。我们还推断,与 CPAP 相比,接受 HFNC 治疗的患者插管风险增加了两倍。