Department of Cardiology Baylor Scott and White The Heart Hospital Plano TX.
Baylor Scott and White Research Institute Plano TX.
J Am Heart Assoc. 2023 Nov 7;12(21):e030774. doi: 10.1161/JAHA.123.030774. Epub 2023 Oct 27.
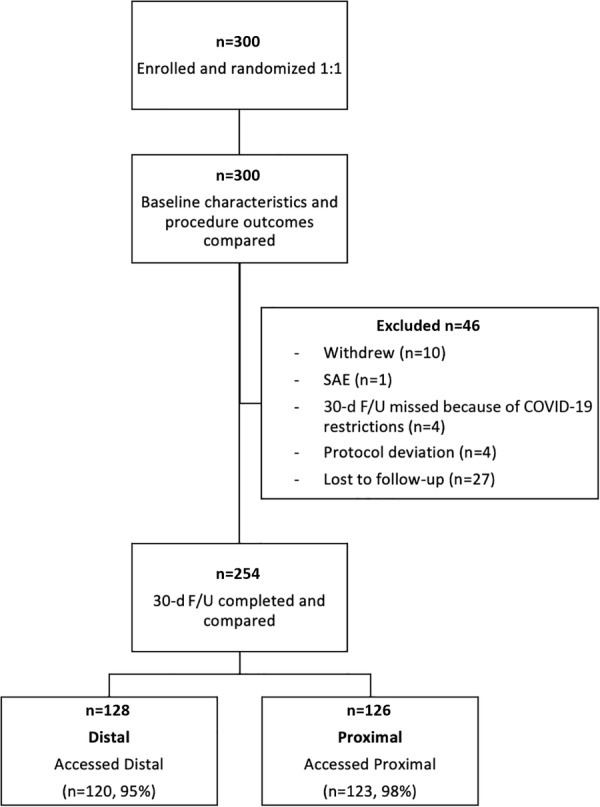
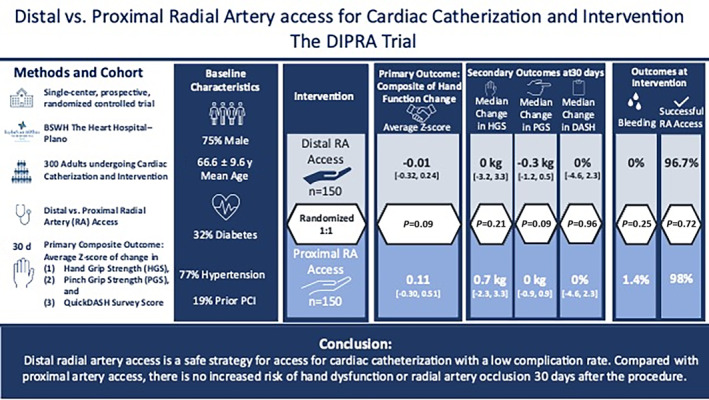
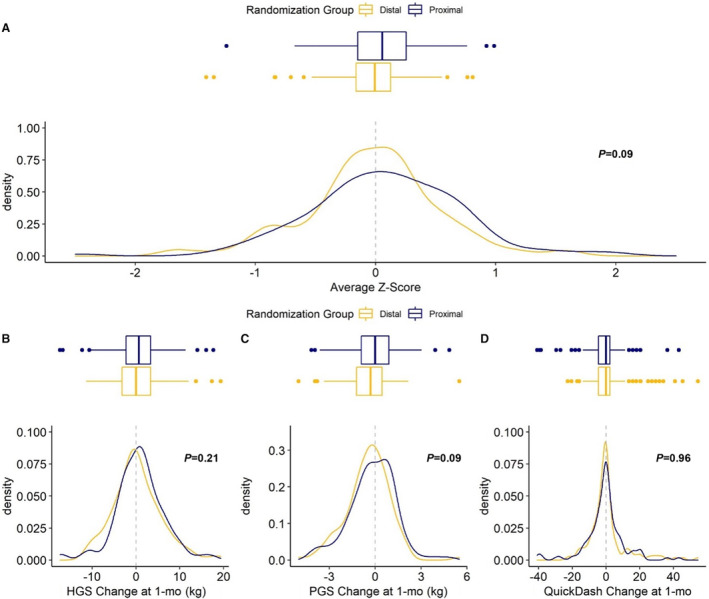
Background Proximal radial artery (pRA) access for cardiac catheterization is safe but can jeopardize subsequent use of the artery because of occlusion. Distal radial artery (dRA) access in the anatomical snuffbox preserves the radial artery, but safety and potential detrimental effects on hand function are unknown. Methods and Results In the DIPRA (Distal Versus Proximal Radial Artery Access for Cardiac Catheterization and Intervention) study, a single-center trial, 300 patients were randomized 1:1 to cardiac catheterization through dRA or pRA. The primary end point of change in hand function from baseline to 30 days was a composite of the QuickDASH (Quick Disabilities of the Arm, Shoulder and Hand) questionnaire, hand-grip test, and thumb forefinger pinch test. Secondary end points included access feasibility and complications; 254 of 300 patients completed follow-up at 30 days; of these, 128 were randomized to dRA and 126 to pRA with balanced demographic and procedural characteristics. Both groups had similar rates of access site bleeding (dRA 0% versus pRA 1.4%; =0.25). Six patients with dRA failed access compared with 2 patients with pRA. Radial artery occlusion occurred in 2 pRA versus none in dRA. There were no significant differences in change in hand function, median hand-grip (dRA 0 [-3.2, 3.3] versus pRA 0.7 [-2.3, 3.3] kg; =0.21), pinch-grip (dRA -0.3 [-1.2, 0.5] versus pRA 0 [-0.9, 0.9] kg; =0.09), and QuickDASH (dRA 0 [-4.6, 2.3] versus pRA 0 [-4.6, 2.3] points, =0.96). There was no significant difference in the composite of hand function between pRA and dRA. Conclusions dRA is a safe strategy for cardiac catheterization with a low complication rate. Compared with pRA, there is no increased risk of hand dysfunction at 30 days. Registration URL: https://www.ClinicalTrials.gov. Unique identifier: NCT04318990.
经桡动脉近端(pRA)入路行心脏导管术是安全的,但可能会因闭塞而危及动脉的后续使用。解剖鼻烟窝内的桡动脉远端(dRA)入路可保留桡动脉,但安全性和对手功能的潜在不利影响尚不清楚。
在 DIPRA(心脏导管术和介入治疗中远端与近端桡动脉入路)研究中,这是一项单中心试验,将 300 例患者随机分为 1:1 接受 dRA 或 pRA 行心脏导管术。主要终点为自基线至 30 天的手功能变化,复合终点为 QuickDASH(手臂、肩部和手残疾快速评估)问卷、握力测试和拇指食指捏合测试。次要终点包括入路可行性和并发症;300 例患者中有 254 例在 30 天完成随访;其中 128 例随机分至 dRA 组,126 例分至 pRA 组,两组患者的人口统计学和手术特征均衡。两组患者的入路部位出血发生率相似(dRA 为 0%,pRA 为 1.4%;=0.25)。6 例 dRA 患者入路失败,2 例 pRA 患者入路失败。pRA 组有 2 例发生桡动脉闭塞,而 dRA 组无桡动脉闭塞。手功能变化、中位握力(dRA 为 0 [-3.2,3.3]kg,pRA 为 0.7 [-2.3,3.3]kg;=0.21)、捏力(dRA 为-0.3 [-1.2,0.5]kg,pRA 为 0 [-0.9,0.9]kg;=0.09)和 QuickDASH(dRA 为 0 [-4.6,2.3]分,pRA 为 0 [-4.6,2.3]分,=0.96)无显著差异。pRA 和 dRA 在手功能复合终点方面无显著差异。
dRA 是一种安全的心脏导管术策略,并发症发生率低。与 pRA 相比,30 天内手部功能障碍的风险没有增加。
https://www.ClinicalTrials.gov。唯一标识符:NCT04318990。