Ceren Akgor Merve, Vuralli Doga, Sucu Damla Hazal, Gokce Saliha, Tasdelen Bahar, Gultekin Fatih, Bolay Hayrunnisa
Department of Neurology and Algology, Faculty of Medicine, Gazi University, Ankara 06560, Türkiye.
Neuroscience and Neurotechnology Center of Excellence (NÖROM), Gazi University, Ankara 06560, Türkiye.
J Clin Med. 2023 Oct 12;12(20):6488. doi: 10.3390/jcm12206488.
Irritable bowel syndrome (IBS) is an under-diagnosed common health problem that impairs quality of life. Migraine and IBS are comorbid disorders that are triggered by foods. We aim to investigate IBS frequency in medication overuse headache (MOH) patients and identify food triggers and food avoidance behavior.
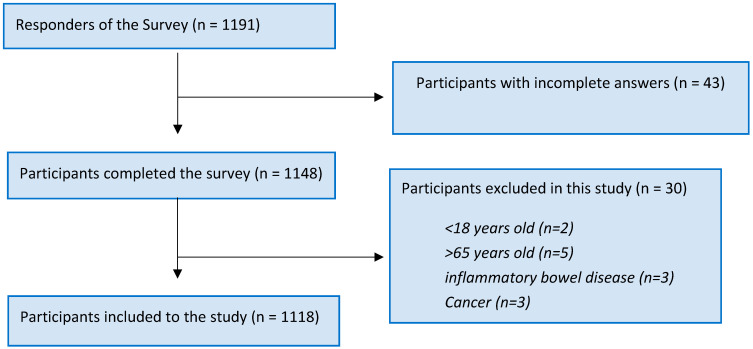
Participants who completed the cross-sectional, observational and online survey were included ( = 1118). Demographic data, comorbid disorders, medications used, presence of headache, the diagnostic features of headache and IBS, migraine related subjective cognitive symptoms scale (MigSCog), consumption behavior of patients regarding 125 food/food additives and food triggers were asked about in the questionnaire.
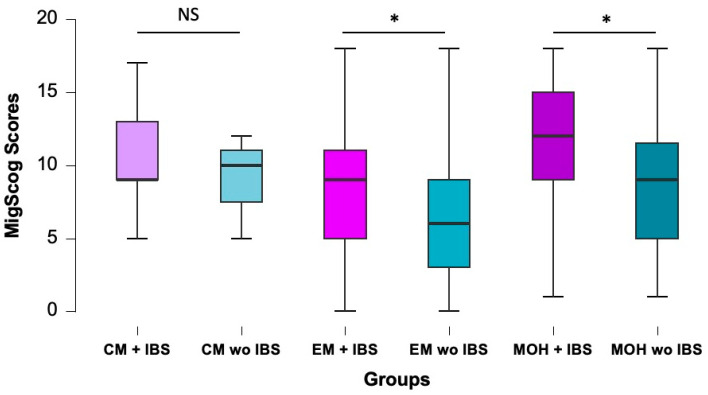
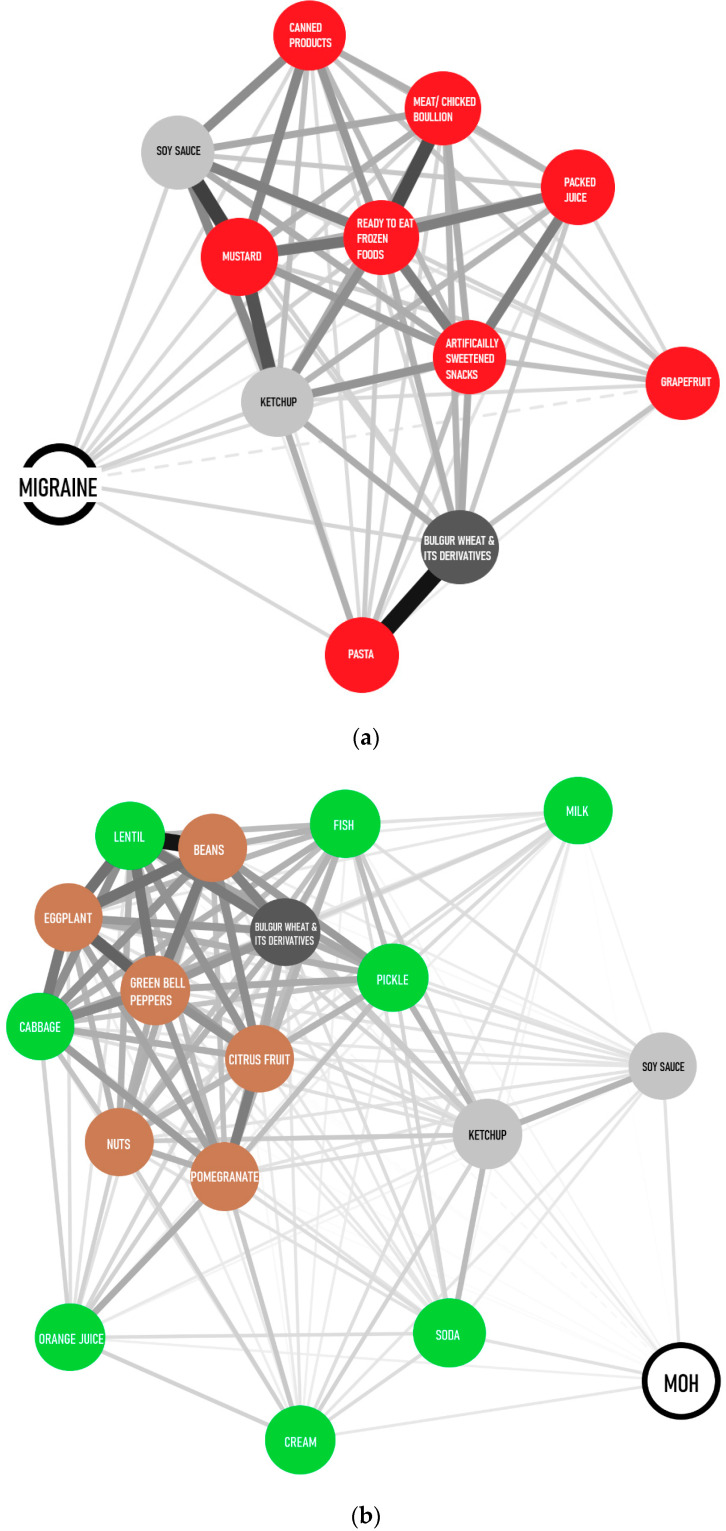
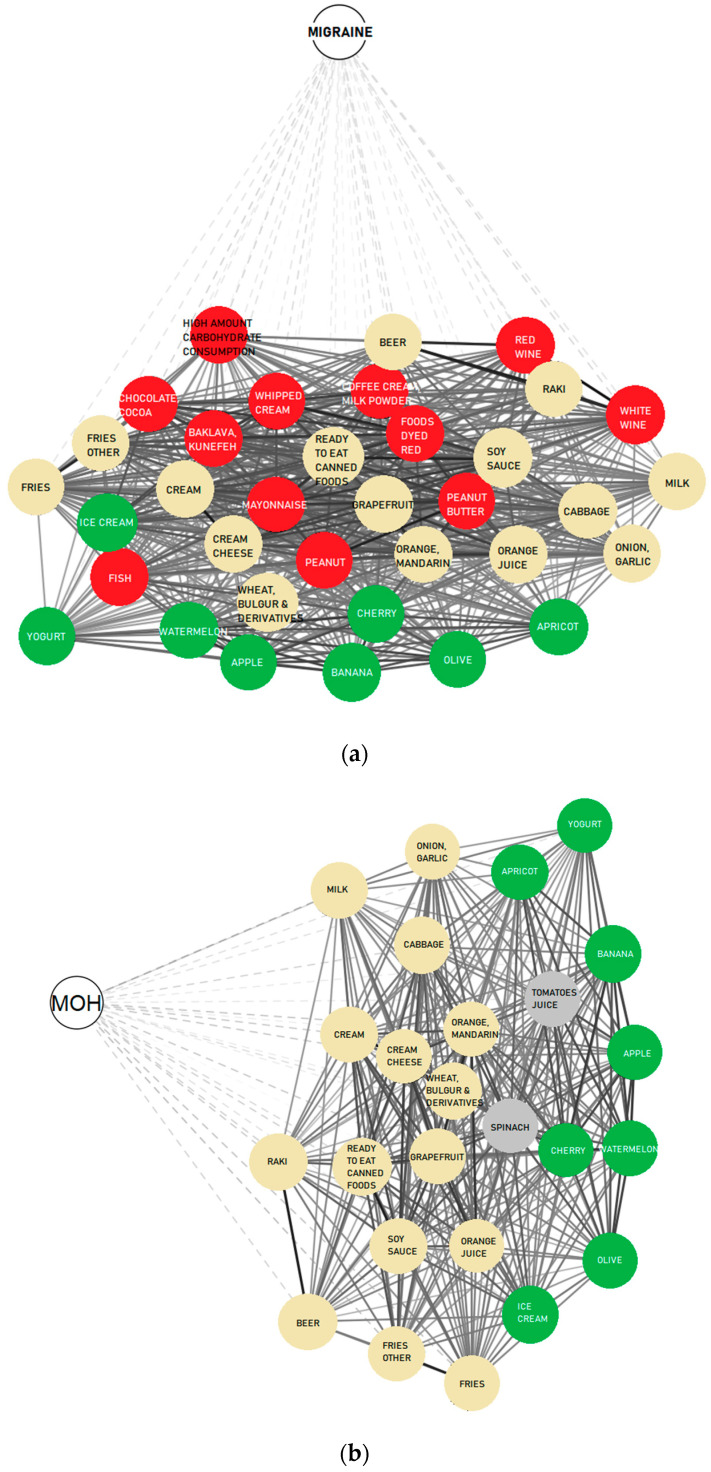
Migraine and MOH diagnoses were made in 88% and 30.7% of the participants, respectively. Non-steroidal anti-inflammatory drugs (NSAIDs) were the main overused drug (89%) in MOH patients. IBS symptoms were present in 35.8% of non-headache sufferers, 52% of migraine patients and 65% of MOH patients. Specific food triggers for MOH patients were dopaminergic and frequently consumed as healthy foods such as banana, apple, cherry, apricot, watermelon, olive, ice cream and yogurt. MigSCog scores were significantly higher in episodic migraine and MOH patients when IBS symptoms coexisted.
The frequency of IBS was higher in MOH patients compared to migraine patients. Coexistence of IBS seems to be a confounding factor for cognitive functions. MOH specific triggers were mostly dopaminergic foods, whereas migraine specific food triggers were mostly histaminergic and processed foods. Personalized diets focusing on food triggers and interference with leaky gut must be integrated to MOH and migraine treatment to achieve sustainable management of these disorders.
肠易激综合征(IBS)是一种诊断不足的常见健康问题,会损害生活质量。偏头痛和肠易激综合征是由食物引发的共病。我们旨在调查药物过量使用性头痛(MOH)患者中肠易激综合征的发生率,并确定食物触发因素和食物回避行为。
纳入完成横断面、观察性在线调查的参与者(n = 1118)。问卷中询问了人口统计学数据、共病、使用的药物、头痛情况、头痛和肠易激综合征的诊断特征、偏头痛相关主观认知症状量表(MigSCog)、患者对125种食物/食物添加剂的消费行为以及食物触发因素。
分别有88%和30.7%的参与者被诊断为偏头痛和药物过量使用性头痛。非甾体抗炎药(NSAIDs)是药物过量使用性头痛患者中主要的过度使用药物(89%)。35.8%的非头痛患者、52%的偏头痛患者和65%的药物过量使用性头痛患者存在肠易激综合征症状。药物过量使用性头痛患者的特定食物触发因素具有多巴胺能性,且常作为健康食物食用,如香蕉、苹果、樱桃、杏子、西瓜、橄榄、冰淇淋和酸奶。当肠易激综合征症状共存时,发作性偏头痛和药物过量使用性头痛患者的MigSCog评分显著更高。
与偏头痛患者相比,药物过量使用性头痛患者中肠易激综合征的发生率更高。肠易激综合征的共存似乎是认知功能的一个混杂因素。药物过量使用性头痛的特定触发因素大多是多巴胺能食物,而偏头痛的特定食物触发因素大多是组胺能食物和加工食品。针对食物触发因素和对肠漏的干预的个性化饮食必须纳入药物过量使用性头痛和偏头痛的治疗中,以实现这些疾病的可持续管理。