Tan Jun Guang Kendric, O'Sullivan Jessica, Wijesuriya Ruwan
General Surgery, St John of God Midland Public and Private Hospitals, Perth, AUS.
Cureus. 2023 Oct 25;15(10):e47634. doi: 10.7759/cureus.47634. eCollection 2023 Oct.
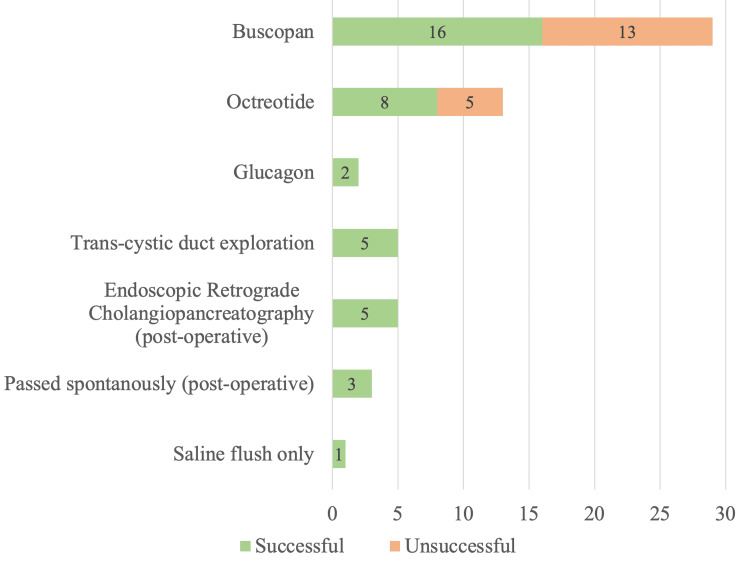
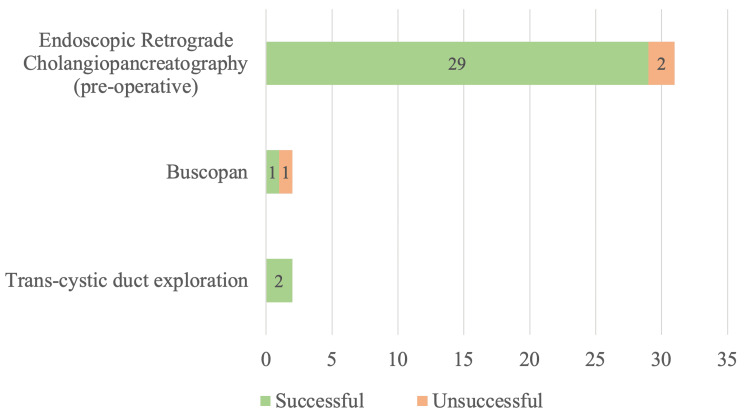
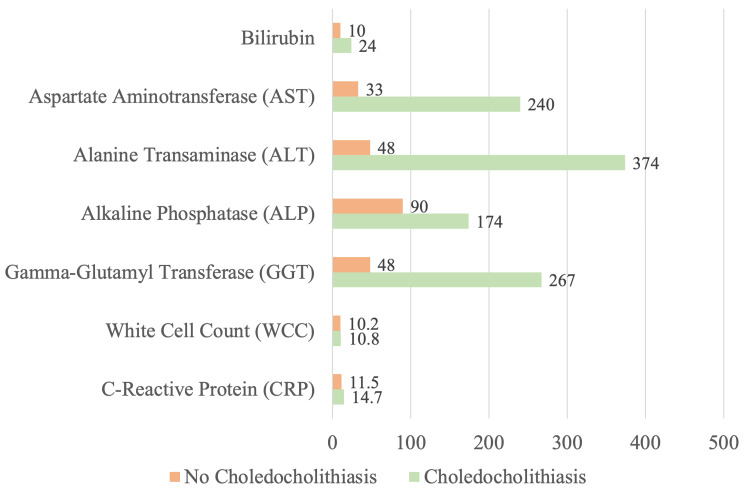
Background Up to 15% of patients with cholelithiasis have choledocholithiasis, with almost 10% not detected pre-operatively. Our study aims to quantify the prevalence of incidental choledocholithiasis during routine intra-operative cholangiogram (IOC), identify the best management pathway, and identify reliable pre-operative factors to predict choledocholithiasis. Methods We conducted a single-centre, retrospective cohort study at St John of God Midland Hospital in Western Australia, Perth, on 880 consecutive patients who underwent cholecystectomies performed by 15 surgeons between January 2, 2020, and December 30, 2021. Results The overall choledocholithiasis rates were 10.6% (93), with 4.0% (35) diagnosed pre-operatively and 6.6% (58) diagnosed during IOC. In all, 50% of incidental choledocholithiasis during IOC were managed with hyoscine butylbromide, with a 55.2% success rate; 22.4% of patients received octreotide, with a 61.5% success rate; and 8.6% of patients underwent trans-cystic bile duct exploration (TCBE) and 8.6% underwent postoperative endoscopic retrograde cholangiopancreatography (ERCP), both with 100% success rates. Choledocholithiasis most commonly presents with gallstone pancreatitis, with a median aspartate aminotransferase (AST) level 7.2 times and alanine transaminase (ALT) level 7.8 times higher than those of patients without choledocholithiasis. Magnetic resonance cholangiopancreatography (MRCP) was the most sensitive in identifying choledocholithiasis with a 66.7% pickup rate. The median common bile duct (CBD) diameter on ultrasound was 8 mm, computerised tomography scans were 11 mm, and MRCP was 9 mm. Conclusion One in 10 cholecystectomies will be complicated with choledocholithiasis, and over half will be incidentally diagnosed during routine IOC. We propose IOC in all cases and hyoscine butylbromide, octreotide, and saline flushes as first-line treatment; if unsuccessful, TCBE is performed. Gallstone pancreatitis, markedly elevated AST/ALT, and imaging showing CBD ≥8 mm may serve as early predictors of choledocholithiasis.
高达15%的胆石症患者合并胆总管结石,其中近10%在术前未被检测到。我们的研究旨在量化常规术中胆管造影(IOC)期间意外胆总管结石的患病率,确定最佳管理途径,并确定预测胆总管结石的可靠术前因素。方法:我们在澳大利亚珀斯西澳大利亚州上帝之约翰米德兰医院进行了一项单中心回顾性队列研究,研究对象为2020年1月2日至2021年12月30日期间由15名外科医生连续进行胆囊切除术的880例患者。结果:胆总管结石的总体发生率为10.6%(93例),其中术前诊断为4.0%(35例),IOC期间诊断为6.6%(58例)。在IOC期间,所有意外胆总管结石患者中,50%采用丁溴东莨菪碱治疗,成功率为55.2%;22.4%的患者接受了奥曲肽治疗,成功率为61.5%;8.6%的患者接受了经胆囊胆管探查术(TCBE),8.6%的患者接受了术后内镜逆行胰胆管造影(ERCP),成功率均为100%。胆总管结石最常见的表现为胆源性胰腺炎,天冬氨酸转氨酶(AST)水平中位数比无胆总管结石患者高7.2倍,丙氨酸转氨酶(ALT)水平高7.8倍。磁共振胰胆管造影(MRCP)在识别胆总管结石方面最敏感,检出率为66.7%。超声检查胆总管(CBD)直径中位数为8mm,计算机断层扫描为11mm,MRCP为9mm。结论:每10例胆囊切除术中就有1例合并胆总管结石,超过半数将在常规IOC期间被意外诊断。我们建议对所有病例进行IOC,并将丁溴东莨菪碱、奥曲肽和生理盐水冲洗作为一线治疗;如果不成功,则进行TCBE。胆源性胰腺炎、AST/ALT明显升高以及影像学显示CBD≥8mm可作为胆总管结石的早期预测指标。